.png)




.webp)
Introduction: Challenges Facing Nurse Practitioners in 2026
Nurse practitioners are the fastest-growing provider group in American healthcare. With more than 461,000 licensed NPs across the US — a figure that grew 7% between 2023 and 2025 alone — and a Bureau of Labor Statistics projection of 40% job growth through 2033, the profession is expanding at a pace that few healthcare roles can match.¹
But growth alone does not resolve the structural challenges that NPs face at every stage of their careers. For students, the path to licensure runs through a clinical education pipeline that is chronically under-resourced. For new graduates, the transition to independent practice is steeper than it should be. For experienced clinicians, the regulatory, administrative, and workforce pressures of 2026 are testing even the most resilient providers.
A 2026 NCSBN Environmental Scan projects that approximately 40% of all nurses plan to leave the profession or retire within five years — an estimated shortfall of 263,870 RNs.⁵ NPs are the profession's most realistic answer to that gap. But training more NPs faster requires solving the placement problem first. And right now, nursing programs are leaving 4,856 seats unfilled each year because clinical placements simply are not available.⁴
Data from NPHub's own placement network makes the supply problem concrete: of 18,314 healthcare professionals who applied to become preceptors, only 2,435 were accepted and completed at least one rotation — a 13.3% acceptance rate driven by strict credentialing standards and schools' specific site requirements.⁸ The preceptor pipeline is not just thin. It is actively filtered, which is why the shortage persists even when clinicians want to participate.
This post is written for both audiences — NP students navigating the early stages of their clinical journey, and practicing NPs managing the daily realities of a profession under pressure. It covers the most significant challenges in clinical education, workforce policy, mental health, technology, and institutional design — and offers actionable solutions at every level.
The challenges are real. So are the pathways forward.
Clinical Placements and Clinical Rotations for NP Students
Why the Preceptor Shortage Exists
The preceptor shortage is not new — but in 2026, it is more acute than at any prior point. The core cause is structural: NP enrollment has grown far faster than the infrastructure needed to support it. Between online-only program expansion, accelerated degree timelines, and the geographic mismatch between where students live and where qualified preceptors practice, the clinical placement pipeline is stretched beyond its natural capacity.²
NPHub's 2026 Research Report puts hard numbers on this dynamic. Of 18,314 clinicians who applied to join the preceptor network, only 2,435 cleared the full credentialing, availability, and site-approval process — a 13.3% acceptance rate.⁸ This is not a gatekeeping problem. It reflects the reality that schools have specific requirements most applicants cannot meet, and that quality supervision demands more than willingness.
The average active lifespan of an NPHub preceptor is just 14.41 months — rising to 19.90 months for those who take on repeat students.⁸ This means the preceptor pool is not a static resource. It requires continuous recruitment just to maintain current capacity, let alone expand it.
Contributing factors include:
- Preceptor fatigue. Experienced NPs and physicians who have supervised students for years are declining to continue, citing inadequate compensation, administrative burden, and insufficient institutional recognition.
- Program proliferation. The number of accredited NP programs has grown significantly in the past decade, producing more students than existing preceptor networks can absorb.
- Geographic concentration. Preceptors cluster in urban and suburban healthcare systems. Students in rural areas, or those enrolled in national online programs without local institutional relationships, face disproportionately limited access.
- Specialty imbalance. Psychiatric mental health, acute care, and geriatrics face more severe shortages than primary care tracks, where the preceptor pool — while strained — remains comparatively larger.
The Real Cost of Last-Minute Cancellations
When a confirmed preceptor cancels — due to a practice change, a family emergency, or an administrative breakdown — the impact on the student is immediate and compounding. Clinical start dates slip. Graduation timelines extend. Financial aid disbursements are affected. Students who are working full-time while completing their programs absorb these delays without a safety net.
In 2026, last-minute cancellations are not edge cases. They are a documented pattern that students must plan for — not hope to avoid.
Backup Placement Strategies That Work
Students who secure their placements successfully treat preceptor searching as a risk management exercise, not a one-shot process. Practical backup strategies include:
- Maintaining a second-tier list of qualified, contacted preceptors at all times during the search process
- Beginning searches four to six months before the intended rotation start date
- Using verified matching services as a parallel track alongside independent outreach — not a last resort
- Notifying your practicum coordinator immediately when a match falls through
NPHub's Perfect Preceptor Promise offers a 100% refund and replacement guarantee — if your placement falls through, you are not starting over alone. Secure your backup plan now with a free NPHub account →
The Specialty Divide: What NPHub's 2026 Data Reveals
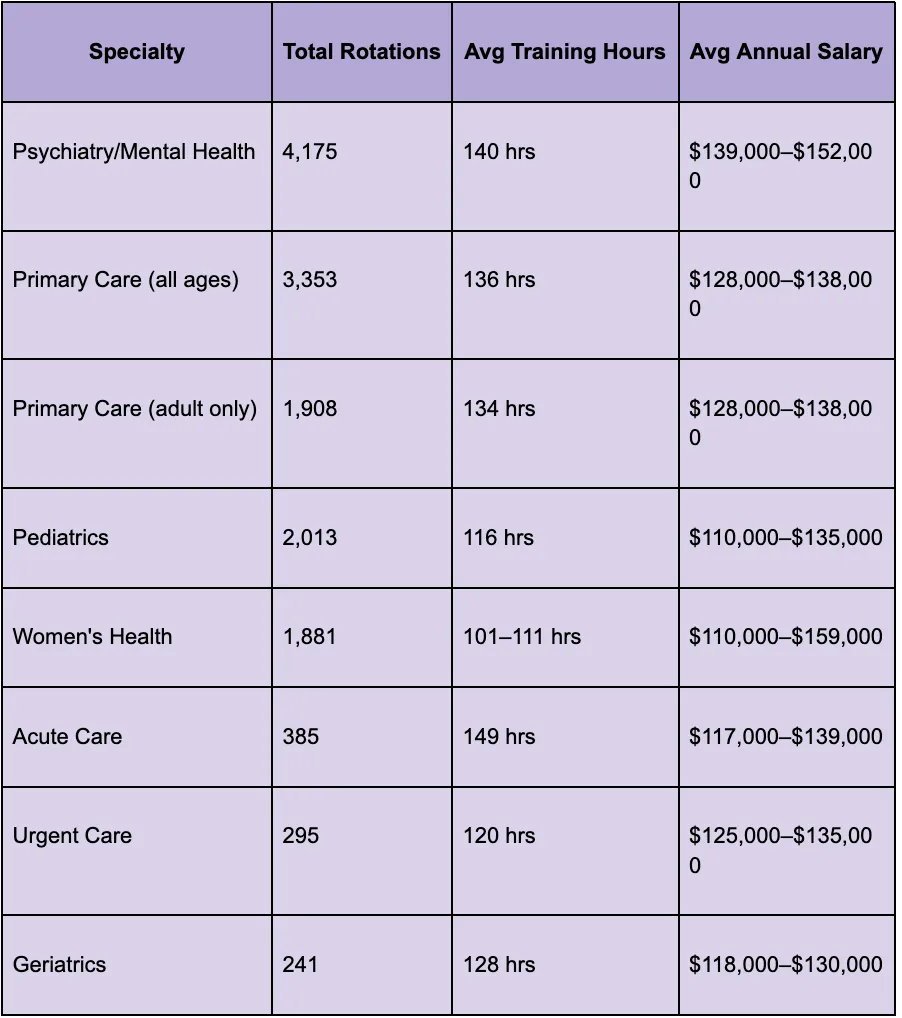
One of the clearest windows into the NP training crisis is specialty-level placement data. NPHub's 2026 Research Report — drawn from more than 14,000 completed rotations across all NP tracks — reveals a pipeline shaped by scarcity, market demand, and a behavioral health crisis that is fundamentally reshaping who becomes a nurse practitioner and how hard it is to get there.
The Full Specialty Breakdown
Psychiatry/Mental Health: The Most In-Demand — and Most Constrained — Specialty
No specialty dominates the NP clinical placement market like Psychiatry/Mental Health. With 4,175 completed rotations, it accounts for nearly 29% of all NP placements in NPHub's dataset — more than any other specialty by a wide margin. PMHNPs now represent 30.7% of all rotations facilitated through NPHub, compared to FNPs at 56.3%.⁸
The career data reinforces why. PMHNPs earn around $139,486 per year — roughly $23,549 more annually than Family Nurse Practitioners. HRSA projects that the supply of PMHNPs will increase 17% between 2016 and 2030, but will still not meet demand for services.⁸ One in five adults in the US lives with a mental illness, and the shortage of psychiatrists continues to create openings that existing PMHNP supply cannot fill.
Students are choosing this track because the need is real, the shortage is persistent, and the career outcome reflects both. But PMHNP rotations average 140 clinical hours — the second-highest of any specialty — and the preceptor pool in psychiatric settings is among the most constrained in the country. High demand, high hours, and a preceptor scarcity that makes placement harder than almost any other track.
Primary Care: The Backbone — and Its Limits
Combined, Primary Care (all ages) and Primary Care (adult only) account for 5,261 rotations — 37% of all placements in NPHub's dataset. A strong preceptor supply of 1,623 across both sub-tracks, consistent career earnings, and the broadest scope of practice make it the most accessible and stable pathway through NP clinical training.⁸
But Primary Care's dominant volume also reflects the ongoing provider gap in primary care access, particularly in rural and underserved communities where NPs are increasingly the primary — and sometimes only — option for patients.²
Acute Care: Hardest Hours, Thinnest Pipeline
Acute Care demands the most average clinical training hours of any specialty — 149 hours per rotation — but ranks third-to-last in volume with just 385 placements. The intensity of the supervisory relationship in high-acuity settings, and the relative scarcity of qualified preceptors willing to take on students in these environments, creates a bottleneck that the volume numbers alone do not capture.⁸ For students pursuing this track, finding a preceptor is often the hardest part of the entire program.
Geriatrics: The Most Underserved Specialty in the Pipeline
Geriatrics presents the starkest concern in NPHub's dataset. Only 241 completed rotations. Only 125 active preceptors nationally. Below-average career earnings relative to time commitment. And this in a specialty facing surging demand as the US 65+ population grows rapidly.⁸
The market has not solved this one — and the training pipeline reflects it. Without targeted intervention at the policy and institutional level, the geriatric care gap will widen precisely as demand for it accelerates.
Preceptor Recruitment, Nurse Educators, and Clinical Placement Partnerships
Incentives That Actually Attract Preceptors
The clinical education system asks a great deal of preceptors and offers comparatively little in return. The 14.41-month average preceptor lifespan in NPHub's network is a direct consequence of this imbalance — supervising students is a real additional demand on top of a full clinical practice, and without meaningful compensation or recognition, attrition is inevitable.⁸
Effective incentive models include:
- Adjunct faculty appointments with access to university library resources, CME credits, and academic career recognition
- Financial stipends — a growing number of programs now offer modest per-hour or per-student compensation to preceptors, particularly in high-shortage specialties
- Formal preceptor appreciation programs that recognize contributions through certificates, annual awards, and program communications
- Loan forgiveness linkages in states that connect preceptor service to NP student loan assistance programs
Academic-Clinical Partnership Models
The most sustainable solution to the preceptor shortage is structural: formalized, maintained partnerships between nursing schools and healthcare systems that create predictable student placement pipelines. Schools that invest in these relationships report significantly lower rates of placement failure and last-minute cancellations.³
Effective partnership models designate clinical education coordinators within health systems, establish rolling affiliation agreements that do not require annual renegotiation, and create shared databases of available preceptors across partner institutions.
Nurse Educator Time Allocation
Faculty time is a finite resource, and in most NP programs, clinical coordination is an add-on responsibility rather than a protected role. The 4,856 unfilled nursing seats reported in April 2026 are a direct consequence of this under-investment.⁴ Institutions that allocate dedicated time — not voluntary effort — to clinical placement coordination see better student outcomes, lower attrition, and stronger preceptor retention.
Balancing Clinical Hours, Work, and Wellbeing for NP Students
Sample Clinical Hours Scheduling Framework
Most NP students are working registered nurses completing their programs while employed full-time. The clinical hours requirement — typically 500 to 750 hours for MSN tracks, 1,000+ for DNP programs — does not pause for the rest of life. A functional scheduling framework looks like this:
- Weeks 1–2: Orientation and schedule alignment with preceptor. Confirm weekly hour targets and shift structure.
- Weeks 3–10: Core rotation period. Target 16–24 clinical hours per week across two to three shifts.
- Midpoint: Formal check-in on competency progress and any schedule adjustments needed.
- Final weeks: Complete documentation, submit hours log, and schedule end-of-rotation evaluation.
Build buffer weeks into your timeline — unexpected conflicts will arise, and a schedule with no margin is a schedule waiting to fail.
Flexible Shift Options: What Employers Can Do
Employers who support NP students through shift-swapping flexibility, protected rotation days, and educational leave policies retain talent at higher rates and build stronger pipelines for their own future NP workforce. Supporting a student's clinical requirements is not a disruption — it is an investment in a future provider.
Self-Care Practices for Students in Clinical Rotations
Burnout does not begin after graduation. For many NP students, it begins during the placement search. The stress of securing clinical hours while managing coursework, employment, and family responsibilities is cumulative and real. Evidence-supported practices that help:
- Scheduled decompression time — even 20 minutes of intentional disconnection between clinical shifts and study sessions measurably reduces cognitive fatigue
- Peer support networks — connecting with other NP students navigating the same challenges normalizes the experience and surfaces practical solutions
- Transparent communication with your preceptor about workload limits — most preceptors respond well to students who advocate for themselves
Clinical Education Quality and Nurse Educators Capacity
The Quality Variation Problem
Not all clinical rotations are equal. The variability in clinical education quality across NP programs is one of the profession's least-discussed challenges. Students at well-resourced programs with strong institutional preceptor relationships receive structured, competency-mapped clinical experiences. Students at under-resourced programs may complete required hours in settings that offer limited teaching, inconsistent feedback, and minimal alignment with their specialty objectives.
This variability has downstream consequences for patient safety, provider confidence, and board certification outcomes.
Faculty Hiring Incentives
The nursing faculty shortage mirrors the preceptor shortage in cause: the compensation gap between clinical practice and academic roles makes faculty recruitment difficult. An experienced NP can earn significantly more in clinical practice than in a tenure-track faculty position. Closing this gap requires targeted institutional investment, including clinical faculty salary adjustments, loan forgiveness for educators, and hybrid clinical-academic role designs that allow faculty to maintain practice while teaching.
Standardized Competency Assessments
Competency-based education — in which students demonstrate specific clinical skills rather than simply logging hours — is the most reliable way to ensure consistent education quality across programs and sites. NPHub's rotation data shows meaningful variation in average training hours by specialty, ranging from 101 hours in OB-only Women's Health rotations to 149 hours in Acute Care.⁸ Programs that map rotation objectives explicitly to NONPF NP Core Competencies, and assess students against them at midpoint and completion, produce graduates who are more consistently prepared for independent practice.²
Regulatory Barriers, Full Practice Authority, and Clinical Practice
Mapping State Practice Models in 2026
As of 2026, nurse practitioners practice under one of three regulatory models depending on their state:
- Full Practice Authority (FPA): NPs can assess, diagnose, treat, and prescribe independently. Currently granted in 27 states and Washington, D.C.
- Reduced Practice: NPs must have a collaborative agreement with a physician for at least one element of their practice.
- Restricted Practice: NPs must practice under physician supervision or delegation for the full scope of their role.
In 2025 alone, more than 50 scope of practice bills were introduced across 19 states, with 33 defeated outright. Legislative momentum toward FPA continues, but progress is uneven and contested.⁶
How Supervision Requirements Restrict Care Access
In restricted and reduced practice states, physician oversight requirements create practical bottlenecks that have nothing to do with clinical competence. NPs in rural areas — where physicians are scarce — cannot practice independently even when they are the only available provider. Patients wait longer. Care goes undelivered. The supervision requirement, in these contexts, is a patient access barrier masquerading as a quality safeguard.
Primary Care's dominant placement volume in NPHub's data — 37% of all rotations — directly reflects this reality: NPs are already functioning as the primary care backbone in underserved communities, and regulatory constraints on their practice are constraints on the patients who depend on them.⁸
Pathways Toward Full Practice Authority
The most effective advocacy strategies combine legislative engagement with outcome data. NPs and professional organizations that publish rigorous, state-specific evidence of NP care quality — patient outcomes, access metrics, cost comparisons — provide legislators with the evidence base needed to support FPA expansion. Joining AANP, participating in state NP association advocacy days, and engaging directly with legislative contacts are the most direct individual contributions a practicing NP can make.¹
Compliance, Licensing, and Multi-State Clinical Practice Considerations
The eNLC and What It Means for NP Mobility
The Enhanced Nurse Licensure Compact (eNLC) allows RNs to hold a single multistate license valid across participating states. However, the APRN Compact — which would extend comparable mobility to nurse practitioners — is not yet universally enacted. As of 2026, NPs who practice or complete clinical rotations in multiple states must navigate individual state licensing requirements, which vary significantly in timeline, cost, and documentation burden.
Steps for Multi-State Licensing
NP students and clinicians managing multi-state practice or rotation requirements should:
- Confirm current compact participation status for each relevant state at the NCSBN website
- Begin licensure applications at least 60–90 days before a needed activation date
- Track renewal timelines for each state license independently — expiration dates rarely align
- Work with your program's clinical coordinator to confirm that your primary state license satisfies supervision requirements at your clinical site
Clinical Practice Challenges: Professional Recognition and Patient Trust
Introducing Your Credentials Effectively
One of the most consistent daily challenges for NPs is establishing professional credibility at the point of care. A clear, confident introduction sets the right tone from the first moment:
"Hi, I'm [Name]. I'm a nurse practitioner — I have a master's degree in nursing and I'm your primary provider today. I'll be doing your full assessment and managing your care."
This introduction is factual, warm, and leaves no ambiguity about the NP's role or authority.
Tracking Outcomes to Demonstrate Value
Individual NPs who track their patient outcomes — chronic disease metrics, preventive care rates, patient satisfaction scores, readmission rates — build an evidence base for their own practice that serves multiple purposes: performance review preparation, job negotiation, and contribution to the broader evidence base for NP-quality care.
Strategies for Team Integration
NPs who invest early in building collegial relationships with physicians, nurses, and administrative staff report significantly lower rates of professional friction. Practical strategies include attending team meetings consistently, communicating clinical decisions transparently, and inviting collaborative consultation on complex cases.
Mental Health: Provider Wellbeing and Patient Care
The Burnout Reality in 2026
A April 2026 analysis by Advisory.com drawing on AMA data shows that burnout rates vary sharply by specialty — driven by workload, administrative burden, and clinical environment.⁷ The drivers are identical for NPs, and no comparable NP-specific breakdown currently exists. What is documented: burnout among advanced practice nurses is at a measurable high in 2026, driven by understaffing, documentation overload, and the emotional weight of managing complex patient populations with inadequate institutional support.⁵
The PMHNP specialty data from NPHub is a vivid illustration of this pressure: 4,175 completed placements, 140 average clinical hours per rotation, a persistent national supply gap, and a patient population — 1 in 5 US adults living with mental illness — that is growing faster than the workforce trained to serve them.⁸ The students entering this specialty are not choosing an easy path. They are choosing to meet a need that the healthcare system has not yet figured out how to fill.
Workplace Mental Health Programs
Healthcare organizations that invest in structured mental health support for their NP workforce — including access to confidential counseling, peer support programs, and formal debriefing after high-acuity cases — report lower turnover, higher engagement, and better patient outcomes. This is not a wellness perk. It is a workforce retention strategy.
Mental Health Training for NPs
All NPs — regardless of specialty — encounter patients in mental health crisis. Programs that embed mental health competency training into core NP curricula, rather than treating it as a specialty-only concern, produce graduates who are more confident and effective across the full spectrum of patient presentations.
Supervision Models for Psychiatric Clinical Rotations
PMHNP students face some of the most constrained preceptor markets in the country. Supervision models that combine in-person preceptorship with structured peer case consultation, faculty-led clinical debriefs, and — where state regulations permit — limited teleprecepted hours can expand access to psychiatric clinical education without compromising quality.
Chronic Disease Management and Evolving Care Models
NP-Led Chronic Disease Management Clinics
Chronic disease management is one of the areas where NP-led care has the strongest evidence base. Patients with diabetes, hypertension, heart failure, and COPD managed by NPs in longitudinal primary care relationships achieve outcomes comparable to physician-managed care — often with higher patient satisfaction scores and lower per-visit costs.² The Primary Care training data in NPHub's report — 5,261 combined rotations, the largest volume of any track — reflects the scale at which NPs are already delivering this care.⁸
Remote Monitoring Integration
Remote patient monitoring — wearables, continuous glucose monitors, blood pressure cuffs connected to care platforms — is becoming standard in chronic disease management. NPs who develop fluency with these tools are better positioned to manage larger panels, identify deteriorating patients earlier, and deliver longitudinal care that is both efficient and genuinely personalized.
Reimbursement Strategies for Longitudinal Care
NPs in independent practice face reimbursement structures designed around episodic, physician-delivered care. Value-based care contracts, chronic care management (CCM) billing codes, and annual wellness visit bundling are the most accessible tools available for NPs seeking to build financially sustainable longitudinal care models.
Technology, Telehealth, and AI in Clinical Practice
The Limits of AI Decision Support
AI diagnostic tools, documentation assistants, and predictive analytics platforms are now present in many clinical settings — and NPs are expected to use them competently and critically from day one. The critical skill is not adopting AI uncritically. It is knowing when to trust it, when to question it, and when to override it. AI tools trained on population-level data can introduce bias in individual patient care — particularly for patients from underrepresented demographic groups.
Telehealth Competency Standards
Telehealth has permanently expanded the scope of where NPs practice. In 2026, telehealth competency is not optional — it is a baseline expectation. Core telehealth skills include: virtual physical assessment techniques, telehealth-specific communication strategies, documentation requirements for virtual encounters, and state-specific prescribing rules for telehealth-delivered care.
Privacy Safeguards for Digital Tools
NPs who use AI-assisted documentation tools, patient communication platforms, or remote monitoring systems must understand HIPAA's application to digital health tools — including which vendor agreements require Business Associate Agreements and what the liability implications of a breach are for independent practitioners.
Hiring Trends, Role Design, and Family Nurse Practitioner Demand
Primary Care Demand for FNP Roles
Family nurse practitioners remain the most in-demand NP specialty by training volume — FNPs account for 56.3% of all rotations in NPHub's dataset.⁸ With 98 million Americans living in primary care shortage areas and physician supply failing to keep pace with demand, FNPs are filling critical gaps across rural and urban underserved markets. In FPA states, FNPs are opening independent practices in communities that have not had a primary care provider in years.
Job Designs That Improve Retention
NP attrition is a measurable problem for healthcare employers — and most of it is preventable. The most common drivers of NP turnover are administrative burden, inadequate autonomy, and compensation misalignment. Employers who redesign NP roles around protected clinical time, reduced documentation overhead, and meaningful career advancement pathways retain their NP workforce at significantly higher rates.
Leadership Pathways for Experienced NPs
The nursing profession would benefit from more NPs in formal leadership roles: clinical director positions, policy advisory roles, program director appointments, and executive healthcare leadership. Experienced NPs who pursue formal leadership training and actively seek governance positions within their organizations and professional associations accelerate this shift for the entire profession.
Policy and Institutional Recommendations to Expand Clinical Placement Capacity
The 4,856 unfilled nursing seats, the projected 263,870-RN shortfall, and NPHub's data showing only 2,435 active preceptors out of 18,314 applicants are not problems that individual students or preceptors can solve alone.⁴˒⁵˒⁸ They require coordinated policy responses at the institutional, state, and federal levels.
Preceptor Tax Credit Programs
Several states have introduced or are considering legislation that would provide tax credits to licensed clinicians who serve as NP preceptors. These programs directly address the compensation gap that drives the 14.41-month average preceptor lifespan in NPHub's network.⁸ NP professional associations in states where this legislation is pending should prioritize its advancement as a workforce development priority.
Shared Clinical Site Networks Between Schools
In markets where preceptor capacity is limited, competing nursing programs pulling from the same small pool of willing preceptors create artificial scarcity. Geriatrics — with only 125 active preceptors nationally and 241 completed rotations — is the clearest example of what happens when no coordination mechanism exists.⁸ Shared clinical site networks expand effective capacity without requiring new preceptors to be recruited.
Funding Increases for Nurse Educator Positions
The nursing faculty shortage is inseparable from the clinical placement shortage. Federal and state funding streams that support nurse educator salary supplements, loan forgiveness for academic nurses, and graduate teaching fellowships for advanced practice nurses are the most direct policy levers available to expand the clinical education infrastructure at scale.
.webp)
Actionable Steps for NP Students and Early-Career Clinicians
Build a Targeted Preceptor Outreach Email
Your first email to a potential preceptor should be under 150 words, personalized to their specific practice, and make a single clear ask:
"Hi [Name], I am a [specialty] NP student at [university], seeking a clinical preceptor for a [X]-hour rotation beginning [month, year]. I came across your work at [clinic/practice] and believe your focus on [specific area] aligns well with my clinical learning goals. I have all required documentation ready — malpractice certificate, immunization records, and affiliation agreement. Would you be open to a brief 10-minute call to explore whether this might be a fit? Thank you sincerely for your time."
If you would rather skip the outreach process entirely, NPHub matches NP students with vetted preceptors across all 50 states — create your free account and find your match in under 20 minutes →
Track Clinical Hours and Rotation Deadlines Proactively
Build a simple tracking system before your rotation begins — a spreadsheet that logs weekly hours completed, cumulative total, required total, and days until your school's paperwork deadline. Students who track proactively identify problems before they become crises.
Create a Competency-Based Learning Plan
At the start of every rotation, sit down with your preceptor and identify three to five specific clinical competencies you want to develop. Write them down. Return to them at your midpoint evaluation. This conversation signals professionalism and gives your preceptor a clear teaching framework.
Join Professional Advocacy and Mentorship Groups
AANP, your state NP association, and specialty-specific organizations like APNA (psychiatric) or AWHONN (women's health) offer mentorship programs, advocacy training, and peer networks that accelerate both clinical development and career growth.
Conclusion: Preparing Nurse Practitioners for 2026 Clinical Practice
The challenges facing nurse practitioners in 2026 are significant — but they are not insurmountable. The preceptor shortage, the burnout crisis, the uneven regulatory landscape, and the rapid pace of technological change are all solvable problems. What they require is coordinated action across clinical education, institutional policy, and professional advocacy.
The numbers tell a story that demands urgency. 4,856 unfilled nursing seats.⁴ A projected 263,870-RN shortfall.⁵ Only 2,435 active preceptors out of 18,314 applicants.⁸ These are not abstractions — they are the direct consequence of under-investment in clinical education infrastructure, and their consequences will be felt by patients, not just students.
For students: Start your preceptor search early, build a backup plan, document your competencies, and do not wait until the last minute to ask for help.
For employers: Protect your NP workforce's time, autonomy, and wellbeing. The cost of replacement far exceeds the cost of retention.
For policymakers and program directors: Preceptor tax credits, nurse educator funding, and shared site networks are not aspirational — they are urgent. The specialty data is clear: Geriatrics is failing. Acute Care is underbuilt. PMHNP demand is outpacing supply. These are policy problems that require policy solutions.
The nurse practitioners being trained today will carry the weight of the US healthcare system for the next 30 years. They deserve a clinical education pipeline that is resourced, supported, and built to succeed.
If you are an NP student navigating the preceptor search right now, you do not have to do it alone. NPHub has helped 9,000+ students secure 14,000+ clinical placements in 9 years — with a 100% placement guarantee and a matching process you can complete in under 20 minutes.
Create your free NPHub account today →
Key Takeaways
- 4,856 nursing seats went unfilled in the past year due to clinical placement unavailability — the placement crisis is now constraining enrollment, not just delaying individual students.⁴
- 40% of nurses plan to leave the profession within five years, creating a 263,870-RN gap that NPs are expected to fill.⁵
- Of 18,314 preceptor applicants, only 2,435 were accepted into NPHub's vetted network — a 13.3% rate that explains why qualified placements are structurally scarce.⁸
- Psychiatry/Mental Health accounts for 29% of all NP placements and carries the highest salary ceiling — but faces one of the most constrained preceptor pools of any specialty.⁸
- Geriatrics has only 125 active preceptors nationally — the most underserved specialty pipeline in a specialty facing surging patient demand.⁸
- Full practice authority remains uneven across states — supervision requirements in restricted states are patient access barriers as much as regulatory requirements.
- Coordinated policy action — preceptor tax credits, shared site networks, nurse educator funding — is the only path to solving the placement bottleneck at scale.
Frequently Asked Questions
1. What is the biggest challenge facing NP students in 2026? The preceptor shortage remains the most disruptive challenge. Nursing programs left 4,856 seats unfilled in the past year due to placement unavailability.⁴ NPHub's data makes the supply problem concrete: of 18,314 clinicians who applied to become preceptors, only 2,435 cleared the full credentialing and availability process.⁸ Students who begin their search early, use verified matching services, and maintain a backup preceptor list are best positioned to navigate this environment.
2. Which NP specialty is hardest to find a preceptor for in 2026? Based on NPHub's 2026 Research Report, Acute Care and Geriatrics present the most constrained preceptor pipelines relative to demand. Acute Care requires the most clinical hours of any specialty (149 average) but has only 385 completed placements. Geriatrics has only 125 active preceptors nationally and 241 completed rotations — the thinnest pipeline of any specialty, in a field facing growing patient demand.⁸ PMHNP placements are high-volume but high-demand, creating meaningful wait times in competitive markets.
3. Why is Psychiatry/Mental Health the most in-demand NP specialty? PMHNPs account for nearly 29% of all NP placements in NPHub's dataset — more than any other specialty. Demand is driven by a documented national behavioral health crisis: 1 in 5 US adults lives with a mental illness, and the shortage of psychiatrists creates persistent openings that existing PMHNP supply cannot fill. HRSA projects that even a 17% supply increase through 2030 will not meet demand. The career outcome reflects this scarcity — PMHNPs earn roughly $23,549 more annually than FNPs.⁸
4. What can NP students do right now if they cannot find a preceptor? First, expand your search radius and specialty flexibility if possible. Second, contact your program's practicum coordinator immediately. Third, use a verified matching service with a defined recovery process. NPHub offers a 100% refund and replacement guarantee and has placed 14,000+ students with vetted preceptors across all 50 states. Start your free account here →
5. How is AI changing clinical practice for nurse practitioners? AI is being integrated into documentation, diagnostics, and patient monitoring workflows at a pace most NP curricula have not yet matched. The critical skill is knowing when to trust AI tools, when to question them, and when to override them — particularly given that tools trained on population-level data can introduce bias in individual patient care.
6. What policy changes would most improve the NP training pipeline? Three interventions have the strongest evidence base: preceptor tax credit programs, shared clinical site networks between programs, and increased federal and state funding for nurse educator positions. The data is clear about where the gaps are most severe — Geriatrics (125 active preceptors nationally), Acute Care (385 total placements), and the broader 13.3% preceptor acceptance rate that defines structural scarcity across all tracks.⁸
Key Definitions
NP Preceptor A licensed, board-certified nurse practitioner, physician, or other qualified clinical provider who supervises an NP student during a required clinical rotation. Of 18,314 clinicians who applied to become NPHub preceptors, only 2,435 — 13.3% — cleared the full credentialing and availability requirements.⁸
Full Practice Authority (FPA) A state designation that allows nurse practitioners to assess, diagnose, treat, and prescribe independently without a required physician collaboration or supervision agreement. As of 2026, 27 states and Washington, D.C. have granted FPA to NPs.
Clinical Rotation A supervised, hands-on learning experience at an approved clinical site, required for NP licensure and board certification. Average training hours range from 101 hours (OB-only Women's Health) to 149 hours (Acute Care) depending on specialty.⁸
Preceptor Shortage A structural deficit in the availability of qualified, willing clinical supervisors relative to the number of NP students requiring supervised hours. In 2026, this shortage is severe enough to leave 4,856 nursing program seats unfilled annually.⁴
PMHNP (Psychiatric Mental Health Nurse Practitioner) A nurse practitioner specializing in psychiatric and behavioral health care. The most in-demand NP specialty in 2026, accounting for 30.7% of NPHub placements with an average salary of $139,000–$152,000 annually.⁸
eNLC (Enhanced Nurse Licensure Compact) A multistate licensure agreement that allows RNs to hold a single license valid across participating states. The APRN Compact — which would extend this mobility to nurse practitioners — is not yet universally enacted as of 2026.
Affiliation Agreement A formal contract between a nursing school and a clinical site authorizing student rotations at that location. Required by most programs before any supervised clinical hours can officially begin. Processing typically takes one to three weeks.
Competency-Based Education An educational model in which students demonstrate specific clinical skills against defined standards rather than simply logging required hours. Tied to frameworks like the NONPF NP Core Competencies.
Burnout A state of chronic occupational stress characterized by emotional exhaustion, depersonalization, and reduced sense of personal accomplishment. Burnout rates among advanced practice nurses are at measurable highs in 2026, driven by staffing shortages, administrative burden, and inadequate institutional support.⁵˒⁷
NCSBN (National Council of State Boards of Nursing) The organization that coordinates nursing licensure across US states and publishes the annual Environmental Scan — a primary regulatory research document tracking workforce trends, licensure data, and policy developments. The 2026 Scan projects a 263,870-RN shortfall within five years.⁵
Article details
- Last updated
April 13, 2026 - Fact-checked by
NPHub Clinical Placement Experts & Student Support Team - Sources and reference
- American Association of Nurse Practitioners (AANP). A Behind-the-Scenes Look at the 2025 Nurse Practitioner Count. November 2025. aanp.org
- NPHub. Top Challenges for Nurse Practitioners and How to Overcome Them. nphub.com/blog/np-practice-challenges
- NPHub. Nurse Practitioner Clinical Sites: Finding the Right Preceptor. nphub.com/blog/np-preceptor-search
- HealthLeaders. Desperate Times Call for Strategic Measures: A Nursing Pipeline Reality Check. April 13, 2026. healthleadersmedia.com
- HealthLeaders. Inside the 2026 NCSBN Environmental Scan: Critical Workforce Trends Every CNO Must Know. April 17, 2026. healthleadersmedia.com
- American Medical Association. Scope of Practice 2025 Legislative Summary. November 2025. ama-assn.org
- Advisory.com. Charted: The Most and Least Burned-Out Physician Specialties. April 28, 2026. advisory.com
- NPHub. The Hardest Rotation to Find (And Why It Pays the Most): Inside the Specialty Divide Shaping NP Training. NPHub Research Report 2026. nphub.com
Find a preceptor who cares with NPHub
Book a rotation.webp)

.webp)


%20(3)%20(2).svg)