.png)



.webp)
TL;DR
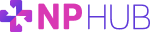
- The bottleneck has shifted. Capacity used to be the dominant question in NP clinical placement — can we find enough preceptors? The harder question now is, do we actually know what's happening across our placements right now? Visibility is the layer underneath capacity, and it's becoming the new operational constraint.
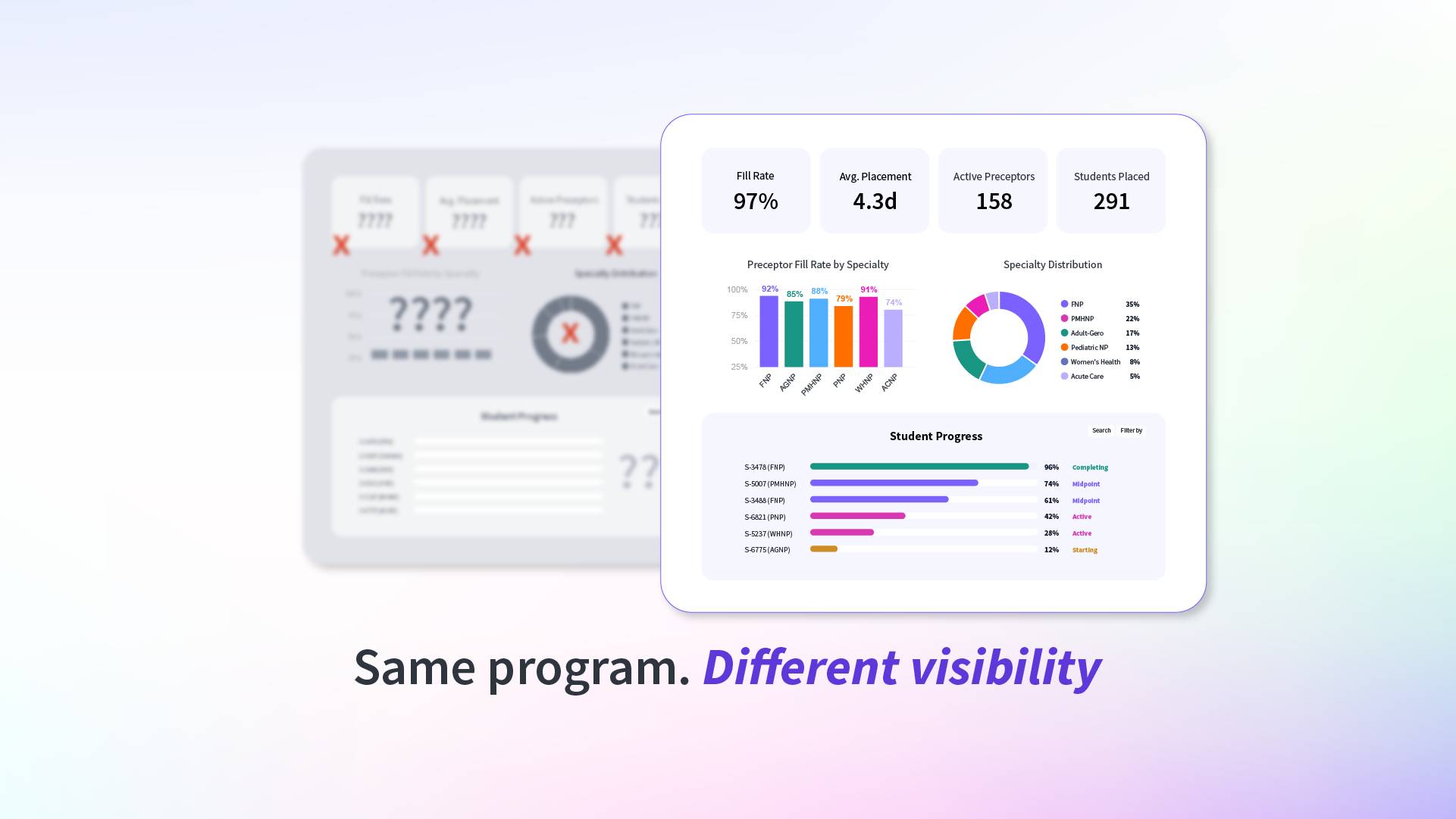
- Faculty burnout and accreditation risk share the same root cause. When no system holds the full picture, faculty become the system, answering questions about preceptor status, affiliation agreements, and site viability that should be answerable at a glance. The same gap that drains faculty time produces the inconsistent documentation that CCNE and ACEN reviewers flag as findings.
- Real visibility operates at four layers. Preceptor-level (still active, still credentialed), site-level (still administratively viable, still appropriate), student-level (hitting clinical requirements, completing direct patient care hours), and program-level (which specialty pipelines are healthy, where time-to-placement is slipping). A gap in one layer surfaces as a problem in another.
- Built-in visibility is a property of how the work is done, not a report produced on demand. Continuous preceptor verification, separate clinical site approval, specialty-level pipeline tracking, and audit-ready records by default turn placement from a reactive scramble into a managed function. NPHub's preceptor recruiting function re-verifies active preceptors and sites every 45 days as the operating standard.
- Want a clear read on where your program's visibility gaps actually sit? The NPHub university partnerships team works through that diagnosis with NP programs every week, across faculty load, accreditation posture, and capacity to grow. Get in touch with our university team.
A few years ago, the dominant question inside most NP programs was straightforward: can we find enough preceptors? Capacity was the bottleneck, and most operational energy went into solving it. That question hasn't gone away but it's no longer the only one, and increasingly, it's not even the hardest one.
The question surfacing now in deans' offices and program director meetings sounds different. Do we actually know what's happening across our placements right now? Which rotations are on track? Which clinical sites are still administratively viable? Which preceptors are currently verified? Which records would hold up if an accreditor asked tomorrow? The shift is subtle, and it points to a different kind of operational problem.
Visibility is the layer underneath capacity. It's what determines whether a program can manage complexity as it grows, defend its records under accreditation review, and protect faculty time from the slow drain of reconstructing information the system should already hold. As nursing schools push more nurse practitioner students into clinical rotations across more specialties, more healthcare systems, and more locations, the cost of operating without that visibility compounds quietly — until a cohort, a review, or a faculty departure makes it visible all at once.
The short version: capacity is what programs are sourcing. Visibility is what tells them whether the sourcing is actually working. This article looks at why that shift is happening now, what placement visibility actually means at the program level, and what it looks like when visibility is built into the clinical placement function rather than reported on top of it.
Want a clearer picture of where your program's placement visibility is straining? The NPHub university partnerships team works through that diagnosis directly with NP programs. Get in touch with our university team.
.png)
Why is Visibility Becoming a Bigger Issue in NP Clinical Rotations?
Visibility is becoming a bigger issue because NP clinical placement has grown more complex (more specialties, more clinical sites, more state-by-state regulatory variation, more accreditation expectations) without a corresponding investment in the systems needed to manage that complexity. Programs that could once track rotations in a spreadsheet now have students placed across dozens of healthcare systems, hospitals, and community clinics, each with its own paperwork, deadlines, and compliance requirements. The result is a quiet operational fog: programs know placements are happening (more or less), but they can't always see the status of any single rotation in real time.
Four shifts are driving the change:
- Enrollment has outpaced informal tracking: Cohort sizes across graduate nursing programs and other nursing practice programs have grown steadily over the past decade. Methods that worked for a 30-student cohort (a shared spreadsheet, a clinical coordinator's inbox, a few key faculty relationships) start to break down at 80, 120, and 200 students.
- Specialty expansion has multiplied workflows: NP programs no longer run one placement process. They run several in parallel, primary care, family nurse practitioner, PMHNP, women's health, pediatrics, adult-gerontology, acute care, each with its own preceptor pool, site requirements, and clinical hour expectations.
- Geographic spread has added regulatory complexity: As distance-learning programs have grown, students are being placed across multiple states, including smaller markets like North Dakota, where preceptor density is thinner and state-level licensure and telehealth rules differ from the program's home state.
- Accreditation expectations have shifted from outcomes to process: CCNE, ACEN, and the American Nurses Credentialing Center are no longer just asking whether clinical hours were completed. Reviewers want to see how placement decisions were made, how preceptors were qualified, how sites were approved, and how oversight was maintained mid-rotation.
A program might have a healthy family practice pipeline and a quietly failing psychiatric mental health pipeline at the same time and not realize it until students start missing rotation start dates. A program might be sound in its process and still fail to defend it under accreditation review, simply because the records weren't kept in real time. The work isn't disappearing. The visibility is.
The compounding effect shows up in the data. Recent industry research found that 30% of program administrators identify clinical placements as the single biggest inefficiency in their operations, more than faculty shortages, technology issues, or scheduling constraints and more than 90% report that placement difficulty directly impacts how their program runs. The work isn't broken at any one step. The visibility connecting the steps is.
What Does "Placement Visibility" Actually Mean for NP Programs?
Placement visibility means a program can answer specific operational questions about its clinical placement program at any moment, which rotations are active, which preceptors are currently verified, which clinical sites are still administratively viable, which students are on track, and which records would hold up under accreditation review. It is the difference between knowing placements exist and knowing how they're performing.
Most programs have some version of each of these data points somewhere. The question is whether they can be assembled into a coherent picture without a week of reconstruction. Real visibility operates at four distinct layers:
- Preceptor-level visibility: Are the experienced preceptors and licensed providers in our network still active, still credentialed, still willing to teach this term? Has anything changed in their license status, scope of practice, or employer restrictions since the last rotation? A preceptor who was a strong match six months ago may not be one today, and without continuous verification, programs find out at the worst possible moment.
- Site-level visibility: Are the clinical settings we approved last year still able to host students? Has the patient population shifted? Are direct patient care opportunities still appropriate for the specialty being placed? Site quality is not static. Staffing turns over, acuity changes, productivity targets tighten. Site-level visibility means knowing which approved sites are still viable, not just which ones are on the list.
- Student-level visibility: Are students hitting clinical requirements, completing direct patient care hours, and meeting the evaluation milestones their program defines? Are clinical experiences progressing in a way that supports the competencies they'll need at graduation? This layer is where most programs have the most data and where that data is most often scattered across faculty notes, preceptor evaluations, and the student's own logs.
- Program-level visibility: Across cohorts and specialties, which placement pipelines are healthy and which are quietly straining? Where is time-to-placement slipping? Which specialty is overdue for new preceptor outreach? Program-level visibility is what allows leaders to make decisions about enrollment, faculty load, and recruiting investment before a shortage becomes a crisis.
The four layers are linked. A gap in one tends to surface as a problem in another. A preceptor whose license lapsed quietly (preceptor layer) becomes a student rotation that no longer counts (student layer), and becomes a documentation gap at the next review (program layer). Visibility at any single layer helps. Visibility across all four is what turns clinical placement into a managed function rather than a recurring fire drill.
Curious where your program's visibility actually sits across these four layers? Talk to the NPHub university partnerships team, we work through that diagnosis directly with NP programs.
.png)
How Do Most Nurse Practitioner Programs Currently Track Clinical Placement Performance?
Most NP programs track placement performance through a combination of spreadsheets, email threads, shared drives, and the working memory of the clinical coordinator. The system works when volume is low and the coordinator is in place. It fails predictably when cohort sizes grow, when the coordinator changes roles, or when an accreditor asks for a full picture of a cohort from three years ago.
The pattern repeats across programs:
- Spreadsheets capture rotations but rarely capture status changes mid-rotation.
- Email threads hold the institutional knowledge and lose it the moment someone leaves.
- Documentation lives in multiple places: the clinical coordinator's inbox, the dean's office, faculty notes, shared drives, the registrar's records.
- When the American Nurses Credentialing Center, CCNE, or ACEN comes calling, the program has to reassemble a picture it should have had in real time.
How Does Poor Visibility Contribute to Faculty Burnout and Accreditation Risk?
Poor visibility shifts the burden of tracking, chasing, and reconstructing placement information onto faculty, work that's invisible in their evaluation, uncompensated in their workload, and incompatible with the academic preparation they were hired to deliver. When no system holds the full picture, faculty become the system. That's where burnout starts.
The pattern is familiar inside most NP programs. Faculty end up answering questions the system should answer: Did that preceptor sign the affiliation agreement? Is that site still active? Is the student's orientation complete? Time meant for curriculum design, nursing education, mentorship, and clinical reasoning instruction goes into administrative reconstruction. The University of Southern California's NP program described the visible tip of this iceberg, a small clinical placement team setting 3 AM alarms to reach sites across time zones, on top of full teaching loads. The work was getting done. The cost was landing on the faculty doing it.
The cost compounds. Faculty turnover takes institutional knowledge with it, and the next person starts from a thinner picture than the last.
Accreditation absorbs the same problem from a different angle. Review has shifted from confirming that clinical rotations happened to evaluating how programs make and document placement decisions. CCNE and ACEN reviewers, along with the Sawyer Initiative's tightening expectations, now want documented, repeatable processes around:
- Preceptor qualification records — current licensure, board certification, scope alignment with program requirements.
- Affiliation agreements — signed, current, matched to active rotations and meeting deadlines.
- Clinical site approval — documented separately from the individual preceptor, with site-level procedures and expectations.
- Ongoing oversight — evidence that conditions were re-verified during the rotation, not just at onboarding.
- Evaluation documentation — direct supervision records, competency assessments, and clinical hour tracking.
Programs without real-time visibility spend the months before review reconstructing these records instead of refining their programs. A program with visibility produces them as a byproduct. A program without it produces them under pressure.
What Does Built-In Visibility Look Like and What Should NP Programs Measure?
Built-in visibility means the recruiting function itself produces the records, status updates, and verification trails programs need without requiring faculty or coordinators to assemble them. Visibility stops being a reporting task and starts being a property of how the work is done.
Five operational elements define what that looks like in practice:
- Continuous preceptor verification rather than one-time onboarding, so that license status, scope of practice, and the clinical environment around experienced preceptors stay current.
- Separate clinical site approval documented independently of individual preceptors, so program leaders can see site health at a glance.
- Specialty-level pipeline tracking so programs know whether primary care, family practice, or psychiatric mental health coverage is healthy before it becomes a crisis.
- Audit-ready records by default so documentation exists because of how the work is done, not assembled retroactively.
- Performance metrics across cohorts, time-to-placement, fill rates, preceptor retention across terms, all visible without manual collection.
This is the operating model NPHub built its preceptor recruiting function around. Board-certified nurse practitioners source and vet every preceptor, NP-to-NP vetting interviews evaluate teaching readiness and clinical fit, credential and license integrity screening runs before placement, clinical sites are approved separately from individual preceptors, and active preceptors and sites are re-verified every 45 days. Visibility isn't a deliverable produced when programs ask for it, it's how the recruiting function operates, supporting timely placement and durable clinical relationships across cohorts.
Once visibility is in place, the question becomes: what should programs actually measure? A small set of operational metrics surface problems early and turn placement from a reactive scramble into a managed function:
- Time-to-placement from request to confirmed rotation, segmented by specialty and geography.
- Fill rate by cohort, what percentage of required clinical rotations were secured on time.
- Mid-rotation disruption rate. How often placements break and need replacement.
- Preceptor retention across cohorts and how many experienced preceptors return for the next term.
- Documentation completeness, what share of active rotations have audit-ready records.
- Student competency outcomes, direct patient care milestones, clinical reasoning assessments, evaluation pass rates that track professional growth and development across the program.
Programs that can produce these numbers are programs that can make decisions about them.
Why Visibility Is Becoming a Competitive Advantage and Why It's No Longer Optional
Programs with real visibility into their clinical placement program move faster, defend their accreditation posture more easily, protect faculty time, and grow enrollment without compromising quality. Visibility creates strategic room to make decisions other programs can't.
Four advantages compound over time:
- Responsible cohort growth: Leaders can see where capacity actually sits before committing to enrollment increases, instead of discovering a shortfall mid-cohort.
- Faster accreditation remediation: When findings emerge, programs already have the documentation infrastructure to respond, not a months-long reconstruction project.
- Stronger clinical partner trust: Hospitals, clinics, and healthcare systems prefer working with programs that communicate proactively, surface issues early, and treat partner relationships as long-term infrastructure.
- Protected program reputation: Students notice when their program seems to know what's happening across their rotations. So do future applicants, professional organizations, and the broader nursing education community.
Capacity is what programs build. Visibility is what tells them whether the building is working, whether the preceptor pipeline is actually deep, whether the documentation actually holds up, whether the faculty are actually protected, and whether the program is actually positioned to graduate competent clinicians into independent practice.
None of the pressures driving this shift are going to ease. Accreditation expectations will continue to tighten. Faculty workload will continue to be a workforce risk. Enrollment demand across NP programs will continue to climb. The complexity of modern healthcare, across specialties, geographies, and care models, will continue to multiply the operational surface area that programs have to manage.
The good news is that the diagnosis is usually clearer than it looks. Most programs already know where their visibility is thinnest, they just haven't had a structured way to address it.
That's the conversation the NPHub university partnerships team has every week with NP programs. If you want a clear read on where your program's visibility gaps actually sit and what built-in tracking would change about your faculty load, your accreditation posture, and your capacity to grow, get in touch with our university team.
.png)
Frequently Asked Questions
What is clinical placement visibility?
Clinical placement visibility is a program's ability to answer specific operational questions about its clinical placement program at any moment — which rotations are active, which preceptors are currently verified, which clinical sites are still administratively viable, which students are on track, and which records would hold up under accreditation review.
It is distinct from clinical placement management, which describes the work of scheduling and coordinating rotations. Visibility is the layer underneath: whether the program can see the status of that work in real time, across preceptors, sites, students, and cohorts.
How can NP programs improve clinical placement tracking?
NP programs can improve clinical placement tracking by moving from spreadsheet-and-email systems to a structured process where verification, documentation, and status updates happen continuously rather than at onboarding. The practical starting points are: centralizing preceptor and site records, separating recruiting from coordination, applying consistent vetting standards across every placement, and tracking a small set of operational metrics across cohorts.
How often should preceptors be re-verified during a rotation?
Preceptors should be re-verified at intervals that catch changes in license status, scope of practice, and clinical setting before those changes disrupt a student's rotation, most structured recruiting functions re-verify every 30 to 45 days. NPHub's preceptor recruiting function re-verifies active preceptors and sites every 45 days as the operating standard.
One-time onboarding verification is insufficient because clinical environments are not static. Staffing turns over, patient populations shift, license status can change, and the scope of practice can narrow. Continuous re-verification protects completed clinical hours and helps secure the audit trail that accreditors expect.
What metrics should a clinical coordinator track for clinical placements?
A clinical coordinator should track six operational metrics that surface problems early: time-to-placement by specialty, fill rate by cohort, mid-rotation disruption rate, preceptor retention across cohorts, documentation completeness, and student competency outcomes. Tracked over time, these metrics turn placement from a reactive scramble into a managed function.
The value is all about decision support. A program watching time-to-placement slip in psychiatric mental health, two cohorts in a row, can invest in recruiting for that specialty before it becomes a graduation-delaying shortage. A program with no metric for that signal finds out at the wrong moment.
How does poor placement visibility affect accreditation outcomes?
Poor placement visibility creates accreditation exposure because it produces inconsistent documentation, missing oversight records, and uneven preceptor qualification trails, the exact patterns CCNE and ACEN reviewers identify as findings. Programs without real-time visibility typically spend the months before review reconstructing records instead of refining the underlying program.
One missing record per cohort isn't a finding. A pattern of incomplete records across cohorts is. Visibility doesn't change the work programs do, it changes whether that work is defensible when accreditors ask.
What's the difference between clinical placement management and clinical placement visibility?
Clinical placement management is the operational work of scheduling rotations, coordinating with preceptors, processing paperwork, and resolving issues as they arise. Clinical placement visibility is the program's ability to see the status of that work, which rotations are on track, which preceptors are verified, and which records are complete, without manually assembling the picture each time.
A program can have strong placement management and weak visibility (the work is getting done, but no one can see how). The reverse is rarer. Strong visibility tends to surface and resolve management gaps; weak visibility hides them until they become crises.
Find a preceptor who cares with NPHub
Book a rotation.webp)


.webp)

%20(3)%20(2).svg)