.png)



.webp)
TL;DR: Building Sustainable Clinical Capacity for NP Programs
- NP enrollment is outpacing clinical placement infrastructure and the semester-to-semester cycle of reactive placement is burning out faculty, delays student graduations, and creating accreditation risk.
- True clinical capacity isn't about available slots. It's the depth, breadth, and reliability of a program's preceptor network, clinical site approvals, and coordination systems, built to compound over time, not reset every term.
- NPHub's Preceptor Recruiting team builds this infrastructure on behalf of NP programs, proactively sourcing, vetting, and maintaining preceptor relationships through a clinician-led process that includes NP-to-NP interviews, credential verification, and 45-day re-verification cycles.
- Programs like Graceland University and USC have used this model to eliminate student stop-outs, expand placement capacity from two-person teams to 50+ dedicated professionals, and free faculty to return to teaching and mentorship.
- If your program is ready to stop restarting every semester and start building clinical capacity that grows with your enrollment, connect with NPHub's university partnerships team to start the conversation.
For most program directors and clinical coordinators, the start of each semester looks the same: sourcing preceptors, securing clinical sites, negotiating contracts, and placing students — often rebuilding the pipeline from scratch.
Faculty are stretched thin. Dedicated teams are small. And the clinical placement process resets every term as though nothing had been built before. The challenge is not a lack of effort. It is a model that does not scale.
NP enrollment has grown significantly; DNP programs alone expanded from 70 students in 2003 to over 41,000 across 433 programs today. Yet clinical capacity has not kept pace. Research shows that 60% of NPs are not currently precepting students, over a third because they were never asked, while provider burnout continues to reduce the available preceptor pool.
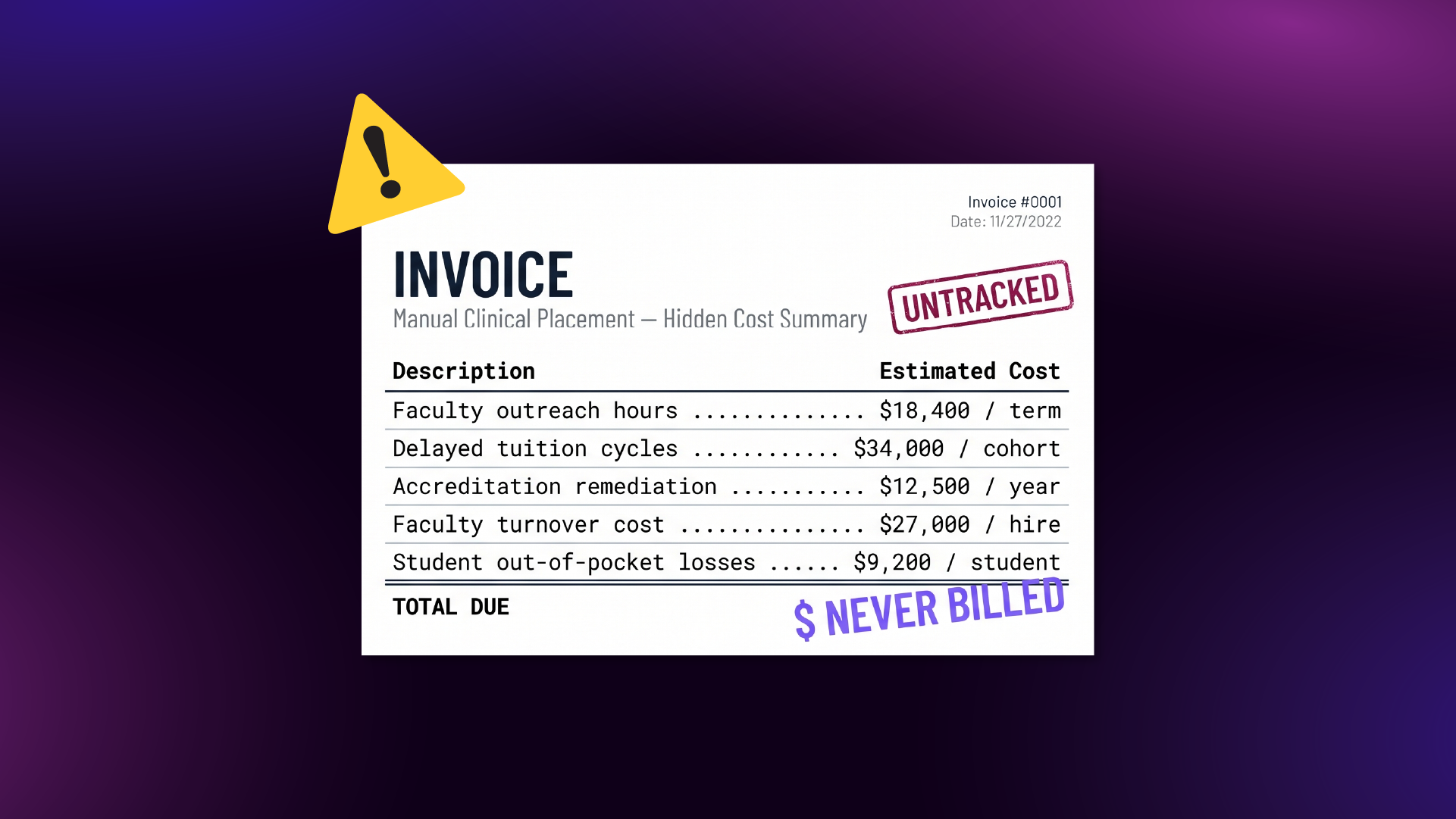
The costs of this reactive cycle are substantial and compounding:
- Student success at risk: Delayed graduations and stop-outs when placements are not secured in time.
- Faculty overextension: Educators diverted from teaching and mentorship into recruitment and contract logistics.
- Accreditation exposure: Inconsistent documentation and oversight gaps that are difficult to sustain through review.
- Uneven clinical experience: Placement quality varies by term and availability rather than by program standards.
This is not a clinical placement problem. It is an infrastructure problem. The programs that are advancing are not simply working harder each semester, they are building sustainable clinical capacity that strengthens over time rather than resetting with every cohort.
That shift is what NPHub's Preceptor Recruiting team is designed to support.
If your program is navigating this cycle, our university partnerships team can help you move beyond it. Connect with our university team to start the conversation.
What "Clinical Capacity" Actually Means for NP Programs
When most program leaders hear "clinical capacity," they think available preceptors and open slots. That's only part of it.
True clinical capacity is the depth, breadth, and reliability of a program's clinical placement infrastructure over time. It's the ability to consistently place students across NP specialties, in diverse clinical settings, with preceptors who are prepared for both clinical practice and teaching, not just whoever happens to be available this term.
That distinction matters because capacity directly shapes the outcomes programs are measured on:
- Accreditation readiness: Accreditation bodies expect traceable records linking clinical experience to competency milestones, documented development of clinical reasoning, and consistent clinical site quality. Programs without sustainable capacity struggle to produce this during reviews.
- Patient safety: When placements are rushed or poorly vetted, students end up in clinical environments that don't support quality patient care or meaningful exposure to diverse patient populations. Research consistently shows that clinical competence, built through structured clinical training with strong preceptor support, is a significant predictor of how successfully nursing students transition into professional practice. Poorly matched placements don't just delay graduation, they undermine the competence development that patient safety depends on.
- Professional growth: The right placement supports professional growth by exposing students to real decision making, capacity assessment across care settings, and the kind of hands-on clinical experience that builds confidence and clinical reasoning, from primary care to the emergency department.
The broader health system context makes this more urgent. Clinical placement saturation is becoming a rate-limiting step to expanding student numbers, and healthcare organizations are not producing available preceptors at the rate NP programs need them. The gap between enrollment growth and placement infrastructure continues to widen.
Programs that treat capacity as a static number will keep falling behind. The ones that build it as a living, compounding system will lead.
Why Semester-to-Semester Clinical Placement Thinking Creates Compounding Risk
In most NP programs, the clinical placement process follows a familiar and exhausting pattern. A clinical coordinator begins the term reaching out to preceptors individually — making calls, sending emails, following up on leads that may or may not convert. When the coordinator's bandwidth runs out, faculty step in, taking on recruitment responsibilities they were never hired or trained for, often while carrying full teaching and advising loads. Meanwhile, students wait — uncertain whether their rotation will be confirmed in time to start the semester on schedule or be delayed.
Then the term ends. And the preceptor relationships that took weeks to cultivate, the affiliation agreements that required rounds of back-and-forth, the clinical site approvals that finally cleared — none of it carries forward in any structured way. The next cohort arrives, and the program starts the entire process over from zero.
This cycle isn't just inefficient. It creates compounding risk across every dimension a program is evaluated on — from accreditation readiness to faculty retention to student outcomes.
The hidden costs most programs absorb without realizing it:
- Lost preceptor relationships: A clinician agrees to take one student, has a disjointed coordination experience, and never volunteers again. The program loses the clinical capacity it has already invested in building.
- Documentation gaps: When placements are inconsistent, the clinical placement process lacks the structured approach and audit trail that accreditation bodies expect. Program leaders can't demonstrate oversight they didn't have the bandwidth to maintain.
- Faculty well-being: Research on nursing faculty burnout confirms what coordinators already feel. A study of 645 nursing faculty found that those working 45+ hours per week and carrying heavy course loads reported significantly higher burnout scores and the workload of chasing placements on top of teaching responsibilities pushes many well past that threshold. Faculty need to teach, advise, and support the development of clinical reasoning, not spend their time sourcing clinical sites and negotiating contracts.
The fundamental problem is structural. When a small, stretched-thin team is responsible for nationwide placement logistics, outcomes suffer — not from lack of effort, but because the model doesn't scale.
Every term a program starts over, it loses ground. Every time it builds on the last; its capacity grows. That's the difference between compounding risk and compounding value — and programs that don't make the shift will feel the gap widen with each passing semester.
Your faculty didn't sign up to be recruiters. Talk to NPHub's university partnerships team about building clinical placement infrastructure that frees your educators to focus on what they were hired to do — while your program's capacity grows every term.
.png)
The Shift: From Filling Clinical Rotations to Building Clinical Infrastructure
There is another way to approach this and it starts with reframing what preceptor recruitment is actually for.
Most NP programs treat placement as a task: find a preceptor, complete the paperwork, move on. NPHub's Preceptor Recruiting team treats it as infrastructure. The goal isn't to fill a slot. It's to build a growing, compounding network of vetted preceptors and approved clinical sites that becomes more reliable and more effective with every term a program partners with us.
Our recruiting team is made up of dedicated nurse practitioners who understand clinical education from the inside, not just the logistics, but the clinical practice, scope, and teaching dynamics that determine whether a placement actually works.
Here's what that looks like in practice.
Turning First-Time Preceptors Into Long-Term Partners
Research consistently shows that what motivates clinicians to precept isn't financial compensation, it's enjoying the work, feeling a professional obligation to give back, and having coworker support and a clearly defined role. What drives them away is the opposite: unclear expectations, poor coordination, and feeling like an afterthought in the process.
NPHub's structured approach is built around this reality. Every preceptor goes through a clinician-led vetting process that includes NP-to-NP interviews, credential and license verification, clinical site approval, and an assessment of teaching readiness, not just clinical qualifications.
But recruiting is only the beginning. Active preceptors are re-engaged every 45 days. This isn't just a compliance checkpoint. It's a relationship touchpoint that confirms practice details remain current, catches changes in patient populations or scope before they become mid-rotation disruptions, and signals to preceptors that their contribution is valued and supported.
The compounding effect is straightforward: preceptors who have positive, well-coordinated experiences come back. They become more effective teachers. Placement outcomes improve term after term, not because the vetting got easier, but because the relationships got deeper.
Expanding Specialty and Geographic Coverage Proactively
NPHub doesn't wait for a student request to trigger a search. Our recruiting team sources and vets preceptors ahead of demand, based on program needs, enrollment trends, and known gaps in specialty or geographic coverage.
This is critical for programs placing NP students in high-demand clinical settings, primary care, psychiatric mental health, emergency departments, and intensive care units across diverse patient demographics and regions. A proactive approach gives programs access to clinical environments and health care organizations they could never reach with a small internal team, expanding their available preceptors across NP specialties and geographies simultaneously.
Planning for Future Cohorts Rather Than Reacting to Current Ones
This is the highest-value outcome of sustainable capacity building. When a program's clinical infrastructure compounds, it can plan enrollment with confidence rather than hoping placements will materialize each term. It can forecast clinical site availability by specialty and term. It can demonstrate to accreditation bodies that its clinical placement process is sustainable and documented — not ad hoc.
And it can protect something harder to quantify but equally important: program reputation. NP programs that can demonstrate strong clinical support attract stronger applicants, retain more students, and maintain their standing with accreditors, creating a cycle where capacity and credibility reinforce each other.
What This Looks Like in Practice
The shift from reactive clinical placement to sustainable capacity building isn't theoretical. Two university partnerships illustrate what changes when an NP program stops starting over each semester and begins investing in clinical capacity that compounds.
Graceland University runs four online NP programs across multiple NP specialties, including Family NP, Psychiatric Mental Health NP, and Adult & Gerontology Acute Care NP. Before partnering with NPHub, their dedicated teams consisted of just two people. They could recruit available in-state preceptors, but sourcing nurse practitioners at clinical sites beyond their home region was functionally impossible. The result: roughly ten NP students per semester were forced to stop out because placements couldn't be secured in time.
After partnering with NPHub:
- Student stop-outs dropped from ten per semester to zero, a direct improvement in student success and on-time graduation.
- NPHub's Preceptor Recruiting team sourced and vetted preceptors exclusively for Graceland's students using a structured approach to credentialing, interviews, and clinical site approval.
- Graceland's placement capacity expanded from a two-person team to a dedicated workforce, giving its nursing students access to clinical rotations across dozens of states.
- Faculty and coordinators reclaimed the bandwidth to focus on clinical training, mentorship, and supporting students through their clinical experience, the work that supports professional growth and program quality.
The University of Southern California faced a different version of the same structural problem. With students scattered nationwide and internationally, faculty carrying full teaching loads found themselves stretched thin — setting 3 AM alarms to coordinate placements across time zones and competing with other programs for the same clinical settings in dense markets.
After partnering with NPHub:
- The unmanageable faculty burden of nationwide coordination was eliminated, allowing educators to return to their core mission of teaching and clinical practice oversight.
- USC expanded from a small clinical team to accessing a dedicated workforce of healthcare professionals focused entirely on preceptor recruitment and placement coordination.
- Students were placed in geographic locations and clinical environments the program had never been able to reach, spanning diverse patient populations and patient demographics from urban primary care settings to locations as remote as Guam.
Program directors and program leaders at both institutions reported the same outcome: more students placed on time, fewer disruptions, and better overall well-being for the faculty who had been absorbing unsustainable workloads.
In both cases, the value wasn't a one-time fix. It was a structural expansion of clinical capacity that carries forward — the network grows, the relationships deepen, and outcomes improve with every term. That's the difference between filling placements and building infrastructure that most programs never get to experience semester to semester.
What Program Leaders Should Be Asking Right Now
The evidence from programs like Graceland and USC points to a clear pattern: sustainable clinical capacity isn't built by working harder within a broken model. It's built by changing the model.
But before making any decisions about partnerships or structural changes, program directors and clinical coordinators should start with an honest assessment of where their program currently stands. The answers will tell you whether your program is moving forward or resetting every term.
- Are we building clinical capacity, or restarting each semester? Do your preceptor relationships, site approvals, and affiliation agreements carry forward in a structured way or does your team rebuild the pipeline from scratch every time a new cohort begins?
- Can our current team sustain this as enrollment grows? If your program admits more students next year, does your placement infrastructure scale with them or does the burden simply increase on the same small group of people?
- Are our faculty focused on clinical training and student development, or on logistics? Every hour an educator spends chasing contracts or calling clinical sites is an hour they're not spending on teaching, mentorship, or supporting students through their practice development.
- Can we demonstrate consistent clinical site quality and oversight for accreditation? If an accreditation reviewer asked today for documentation showing how your program evaluates, approves, and monitors clinical sites across terms, would the answer reflect a sustainable system or a series of one-off decisions?
- Do we know where our outcomes stand and are they improving? Placement rates, on-time graduation, student satisfaction, and preceptor retention are all measurable. Programs that track these metrics term-over-term can identify gaps early and demonstrate progress. Programs that don't navigate blindly.
Start Building Clinical Capacity That Grows With Your Program
The NP programs that will lead over the next decade are the ones that build clinical capacity now, systematically, proactively, and in a way that compounds with every term.
Every preceptor relationship that carries forward is an asset. Every clinical site that is vetted, approved, and maintained is an infrastructure that the next cohort can rely on. Every term that builds on the last moves a program further from the reactive cycle that holds so many back — and closer to the kind of predictable, scalable outcomes that accreditors, students, and faculty all need.
That's the work NPHub's Preceptor Recruiting team does every day, on behalf of NP programs that are ready to stop filling placements and start building.
If your program is ready to make that shift, our university partnerships team is here to start the conversation. Connect with our team to explore what sustainable clinical capacity planning looks like for your program.
Frequently Asked Questions
What is clinical capacity in the context of NP education?
Clinical capacity is more than available preceptors and open slots. It's the depth, breadth, and reliability of a program's clinical placement infrastructure over time — including vetted nurse practitioners serving as preceptors, approved clinical sites across NP specialties and geographies, and sustainable coordination systems that carry forward term after term.
How does clinical placement quality affect patient safety?
When placements are poorly matched or rushed, students end up in clinical environments that don't support quality patient care or meaningful clinical training. Structured placements with vetted preceptors ensure students develop competence in medical decision making, capacity assessment, and patient education — skills that directly impact patient safety. Research shows that clinical competence built during rotations is a significant predictor of how successfully nursing students transition into professional roles as registered nurses and nurse practitioners.
How does NPHub help programs build sustainable clinical capacity?
NPHub's Preceptor Recruiting team operates as an embedded extension of a program's clinical placement team. Our recruiters are dedicated nurse practitioners who proactively source, vet, and develop preceptor relationships using a structured approach — NP-to-NP interviews, credential verification, clinical site approval, and 45-day re-verification cycles. Rather than filling slots reactively, NPHub builds a compounding network that grows stronger every term, helping programs expand coverage, reduce faculty burnout, improve outcomes, and demonstrate consistent oversight for accreditation.
How do workforce planning and capacity management affect NP program outcomes?
Programs that forecast clinical site availability by specialty and term, track preceptor retention, and monitor placement outcomes over time can make informed decisions about enrollment and resource allocation. Without this data-driven approach, programs risk overextending their infrastructure, exposing gaps during accreditation, and delivering inconsistent clinical experiences across cohorts. NPHub supports this by providing program-level visibility and building infrastructure that scales with enrollment.
Find a preceptor who cares with NPHub
Book a rotation.webp)


.webp)

%20(3)%20(2).svg)