.png)



.webp)
TL;DR
- The instinct to fix placement with more speed and less friction is backward. Many nurse practitioner clinical placement challenges aren't caused by scarcity alone; they're caused by the rush to fill clinical placements fast, which is exactly what produces rejected rotations, mid-rotation surprises, and thin documentation.
- Placements rarely fail at sourcing. They fail downstream. A preceptor saying yes is the start, not the finish. The expensive failures happen later: rejected at school approval, collapsing mid-rotation, or completing with paperwork too thin to defend during a CCNE or ACEN review.
- More preceptors isn't more capacity. Volume is how many available preceptors a program can name; capacity is how many will survive approval, support the required clinical hours, and hold to completion. Open-listing preceptor matching services add the first and leave the second to the program.
- Strict vetting is the standard worth demanding. Clinician-led oversight, a structured NP-to-NP interview, license-integrity screening, separate clinical site approval, and ongoing re-verification confirm fit before a placement is offered, not after it breaks, and protect the graduation timeline in the process.
- Vetting and accreditation readiness are the same investment. When sourcing follows a repeatable standard, the records reviewers expect (preceptor qualifications, approved clinical sites, signed affiliation agreements, ongoing oversight) exist by default instead of being assembled under audit pressure.
- If your program is feeling the gap between cohort size and clinical capacity, this is the exact problem the NPHub university team works on with NP programs. Book a call with our university partnerships team to map it to your cohort size, specialty mix, and graduation timeline.
For most nurse practitioner programs, the math stopped working a while ago. Each cohort arrives a little larger than the last, and the number of confirmed clinical rotations never quite catches up. Faculty and clinical coordinators feel it first: more nurse practitioner students than placements, a calendar that keeps tightening, and a clinical placement process that somehow feels harder every term instead of easier.
The instinct, understandably, is to push for volume. Find more preceptors. Move faster. Strip out the friction. If placements are the bottleneck, the thinking goes, then the fix is simply more placements, secured more quickly, with fewer steps in the way.
This piece makes the opposite case. A lot of what programs experience as nurse practitioner clinical placement challenges isn't caused by scarcity alone. It's caused by the rush to fill clinical placements as fast as possible, because speed without scrutiny is exactly what produces the rejected rotations, mid-rotation surprises, and thin documentation that make the next cohort even harder to place. The friction most programs are trying to eliminate is, in many cases, the part doing the actual work.
So we'll look at three things: what actually breaks in a placement (and why it's rarely the part everyone blames), why faster is so often more expensive in the end, and what changes when vetting is treated as the foundation of the process rather than an obstacle to it.
If your program is already feeling that gap between cohort size and clinical capacity, this is the exact problem the NPHub university team works on with NP and PA programs. You can get in touch whenever a conversation would be useful.
Why do clinical rotations feel harder than they should?
Clinical placements feel harder than they should because most programs are optimizing for the wrong finish line. The instinctive goal is to fill a rotation: find a name, confirm a site, lock the dates. But the real goal is to secure a placement that survives school approval, runs cleanly to completion, and leaves behind documentation a program can defend later. Those two goals look similar from a distance, and chasing the first one quietly undermines the second.
The preceptor shortage is real, and it deserves to be named plainly. NP enrollment has grown far faster than the pool of clinicians willing to teach, and the same nurse practitioner preceptors get approached by multiple programs every term. A widely cited analysis of the NP preceptorship shortage found that 61% of surveyed students rated finding a preceptor an eight, nine, or ten on a ten-point difficulty scale. The scarcity is not imagined, and no amount of process design makes a thin market thick.
But scarcity is not the whole story, and treating it as the whole story is part of why the problem feels intractable. If the shortage were the only variable, programs with reasonable access to clinical sites would not still be losing rotations late in the term. They do, and the reason is structural: when finding preceptors becomes a race against the calendar, the clinical placement process starts rewarding speed and availability over fit. A preceptor who is reachable and willing gets confirmed quickly, even when the match is loose. In practice, "loose" usually means one of a few things:
- The specialty or scope doesn't quite line up with what the rotation requires
- The clinical site can host a student on paper, but isn't really set up to support one
- The patient population won't give the student the clinical experiences that the course is built around
Each of those gaps is invisible at the moment of booking and expensive afterward. A rotation built on availability rather than fit is the kind that gets questioned during school approval, strains halfway through, or generates records too thin to hold up. So the program does the work twice: once to fill the slot, and again to repair it. Multiply that across a cohort and the math turns punishing. The effort that should have produced enough preceptors instead produces a backlog of near-misses that each need rescuing.
The harder a program pushes on speed to relieve the pressure, the more fragile placements it creates, and fragile placements are what generate the next wave of pressure. The feeling that placement keeps getting harder is real. It is about how few preceptors exist and also about a process that treats every available preceptor as a solved problem the moment they say yes.
What actually makes a clinical placement fail?
Most clinical placements don't fail at the point of sourcing. They fail downstream, after a preceptor has already said yes. The match looks secured, the dates are on the calendar, and then it comes apart in one of three predictable ways: it gets rejected during school approval, it collapses partway through the rotation, or it runs to completion but leaves behind paperwork too thin to defend later. Sourcing gets the attention because it's the visible struggle. The failures that actually cost programs the most happen quietly, after the hard part looks done.
The three failure modes are worth naming individually, because each one traces back to a specific gap that vetting is supposed to close:
- Rejection during school approval: A placement confirmed in good faith stalls upon school review. The preceptor's credentials don't fully align, the affiliation agreement isn't in place, or the clinical site was never formally vetted as approved rather than simply willing. The rotation was real; it just couldn't clear the program's own clinical requirements once the school paperwork came due.
- Mid-rotation collapse: The placement clears approval and begins, then destabilizes. The preceptor's schedule shifts, the practice restructures, the patient population does not match what the course requires, or the site can no longer host a student. Because nothing was rechecked after the initial yes, the change only surfaces when it disrupts the student, usually with clinical hours already partly logged and few good options left.
- Undocumented completion: The least visible failure, and often the most expensive. The rotation ends, the student completes the hours, and, on the surface, everything works. But the records are incomplete: no current license verification on file, no signed site approval, no evidence of oversight during the rotation. One thin file is a clerical issue. A pattern of them across cohorts is exactly what surfaces as a finding during a CCNE or ACEN review.
The thread connecting all three is that none of them are sourcing problems. They're fit-and-verification problems wearing a sourcing costume. A placement built solely on a preceptor's willingness carries each of these risks invisibly. A placement built on confirmed fit, an approved site, and complete documentation has already retired them before the rotation starts.
This reframes what "securing a placement" actually means. Finding qualified nurse practitioner preceptors is the beginning of the work, not the end of it. The placement isn't truly secured when someone agrees to precept. It's secured when the program can be confident the rotation will survive approval, hold together start to finish, and stand up to scrutiny long after the student has moved on, protecting both the graduation timeline and the program's standing in the same motion.
Does finding more nurse practitioner preceptors actually solve the shortage?
No. Adding more preceptors only helps if they're the right ones, and most efforts to relieve the shortage prioritize volume over fit. A preceptor who isn't a clinical match for the rotation, or whose site can't actually host a student, doesn't add capacity. It adds a placement that will fail later. Counting that as a solved rotation is how programs end up with a pipeline that looks full and performs empty.
This is the distinction that gets lost: volume and capacity are not the same thing. Volume is how many available preceptors a program can name. Capacity is how many of those will survive school approval, support the required clinical experiences, and hold together to completion. A list of fifty potential preceptors with no vetting behind it is volume. A smaller set of confirmed, fit-checked, site-approved matches is capacity. The first number is bigger and the second number is the one that protects the cohort.
It's worth being precise about why the shortage is genuinely hard, because the fit problem sits on top of a real supply constraint. The research is consistent here:
- Demand is structurally outrunning supply. NP student enrollment is projected to grow roughly 40% by 2031, while the preceptor pool stays largely flat.
- Programs aren't only competing with each other. In saturated regions, NP students compete with medical, PA, and other health-discipline students for the same clinicians, and many preceptors already teach for multiple schools at once.
- The thinnest pools are exactly where fit matters most. Specialty rotations like psychiatric mental health and women's health, and placements in rural areas, have the fewest slots, so a loose match there is the hardest one to repair.
Where the marketplace model breaks down
This is where open-listing models show their limits. A lot of clinical placement services and preceptor matching services operate as directories: they surface a name, make the introduction, and step back. The connection happens, but the judgment doesn't. Whether the scope, specialty, patient population, and site are right for the rotation gets handed back to the people least equipped to assess it, the student and the program coordinator, usually under a deadline.
Used that way, a preceptor matching tool or NP preceptor finder is really a faster way to find a preceptor, not a way to confirm the match is sound. It compresses the search. It doesn't close the verification gap. And for the specialties where most preceptors are already stretched thin, a quick introduction to a willing-but-loose match is precisely the placement that comes apart in week six.
This is the gap a true clinical capacity partner is built to close, vetting fit and approving the site before a placement is offered, not after it fails. If your program is weighing whether your current placement support actually verifies fit or just makes introductions, the NPHub university team can walk through where the line falls. Get in touch today.
Is faster placement always a better placement?
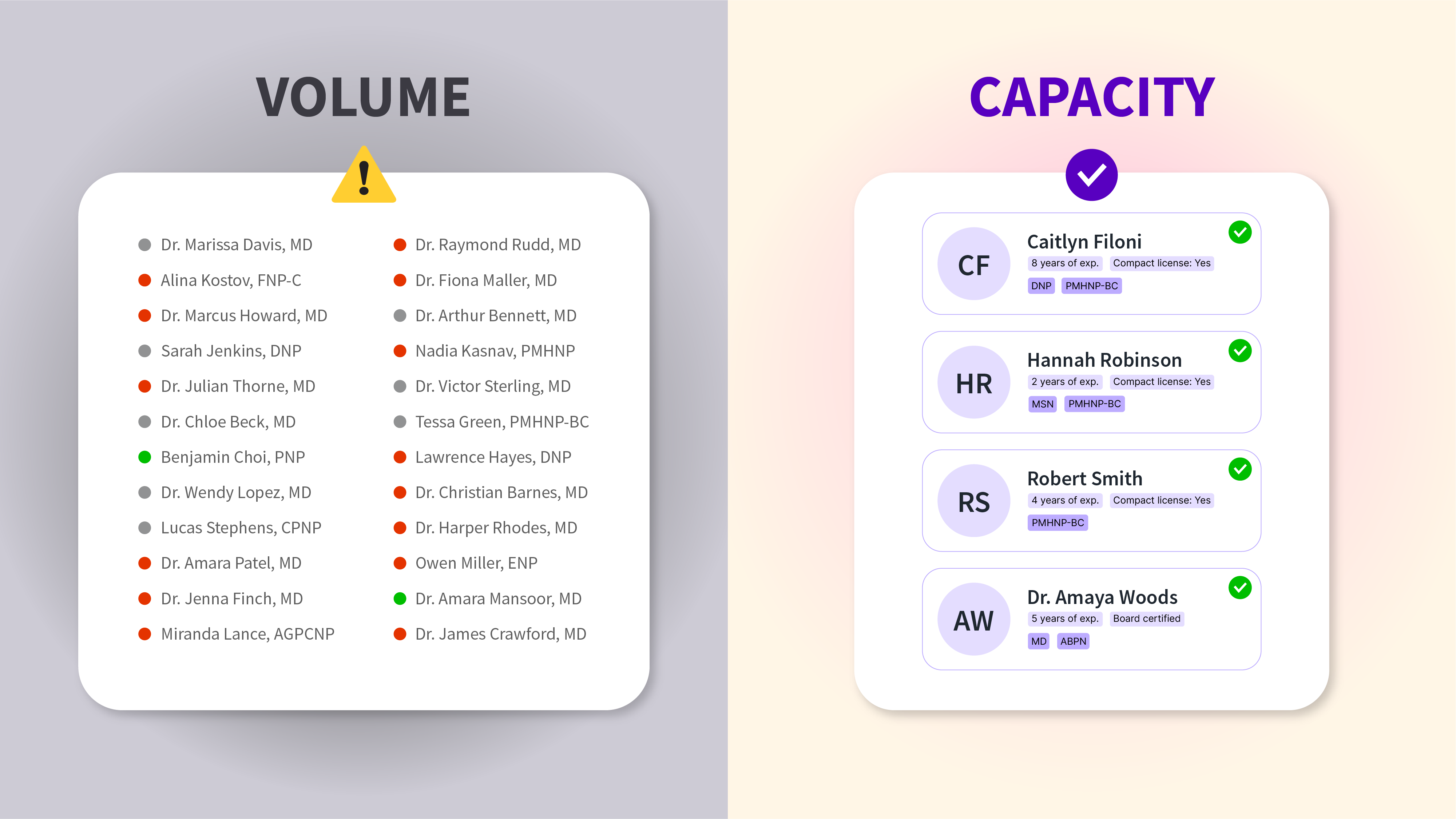
Faster is not free. When a clinical placement process optimizes for speed above everything else, the cost doesn't disappear. It moves downstream and reappears as rejected rotations, delayed graduations, and students paying out of pocket to fix a problem the system created. Speed that skips fit isn't a shortcut. It's a tax that gets collected later, with interest.
The clearest sign a model is straining is who ends up absorbing the work. When programs run out of internal capacity, the sourcing burden quietly shifts to the people with the least leverage to carry it:
- Students start cold: Many NP students start the search themselves, making calls to clinics that don't allow students or never reply. More than half of those outreach attempts go unanswered, and the term starts anyway.
- The financial burden lands on the student: When self-placement fails, students often turn to paid clinical placement assistance out of pocket, sometimes on a payment plan, in addition to tuition. A structural program responsibility becomes a personal expense.
- The mismatch problem compounds: Students in thin specialties or rural areas, who can least afford to travel or wait, are the ones most often left scrambling when a rushed match falls through.
None of this is what programs or students expect when they picture a streamlined process. The promise of speed is a stress free experience: a placement secured quickly and quietly, so the student can focus on clinical learning instead of logistics. The reality of speed-without-fit is the opposite: a placement secured quickly and loudly, with the noise arriving a month later when it breaks.
The goal is always a placement that holds. When fit and verification come first, speed becomes a byproduct of a working pipeline rather than a gamble taken against the calendar. A program isn't slow because it vets. It's slow because it has to keep redoing placements it rushed.
What does a strict preceptor vetting process actually involve?
A strict preceptor vetting process evaluates three things, not one: the clinician, the clinical site, and whether the fit holds over time. A license check confirms someone is allowed to practice. It says nothing about whether their scope, specialty, and setting will support the rotation a student actually needs. That second judgment is a clinical one before it is an administrative one, which is why serious vetting is led by people who have practiced, not by a form or an algorithm.
In practice, a rigorous standard has five components. NPHub's process is built around them, and they translate cleanly into what any program should expect from real vetting:
- Clinician-led oversight: Sourcing and evaluation are handled by an internal team of board-certified nurse practitioners, not third-party reviewers. Because they have worked in similar settings, they can judge whether a preceptor's practice and patient population fit clinical education, the kind of call experienced preceptors are equipped to make and a credential checker is not.
- A structured NP-to-NP vetting interview: Every prospective preceptor completes a focused 20-minute conversation with a board-certified NP. It confirms practice location, scope of practice, NP specialty alignment, daily workflow, and whether the environment supports real hands-on patient care rather than observation only. This is where loose matches across primary care, family practice, women's health, acute care, and urgent care get caught before they become a placement.
- Credential and license-integrity screening: Board certification and an active, unrestricted license are verified, and any disciplinary action, restriction, or unresolved issue is automatic disqualification. There is no version of "qualified preceptors" that skips this step.
- Separate clinical site approval. The site is vetted on its own, not assumed to be fine because the preceptor is. Many disruptions come from the site, not the individual, so administrative readiness to host a student is confirmed independently.
- 45-day re-verification: Vetting doesn't stop at onboarding. Active preceptors and sites are re-checked every 45 days, because schedules, scope, and patient populations shift mid-rotation, and a match that was sound in week one may not be by week six.
The goal is to evaluate fit and readiness to teach, not just availability. It's the difference between confirming someone can precept and confirming this nurse practitioner preceptor will give this student the clinical experiences and clinical skills the course is built to develop. Precepting NP students well is a teaching act, and vetting for various specialties has to account for that.
How does preceptor vetting protect a program's accreditation standing?
Vetting and documentation are the same work done well. When sourcing follows a repeatable standard, the records accreditors expect aren't a separate project assembled under pressure before a site visit. They're the natural byproduct of how each placement was secured in the first place.
CCNE and ACEN reviewers have converged on a predictable set of questions, and the Sawyer Initiative raised the bar on all of them, especially for distance programs. Reviewers want to see:
- How preceptor decisions are made and documented, including qualifications and clinical experience
- Evidence that clinical sites were formally approved, not merely used
- Current, signed affiliation agreements matched to active rotations
- Proof of ongoing oversight across the full length of the rotation
A program running ad-hoc sourcing can usually produce some of this, some of the time. The exposure isn't one missing file; it's the pattern that emerges across cohorts when no single standard governs the records. A structured vetting process closes that gap quietly, because each of those four items is generated as placements happen rather than reconstructed afterward.
What should NP programs look for in clinical placement services?
The question that actually separates a partner from a vendor is "how do you decide a preceptor and site are right for this rotation, and can you prove it later?" A capacity partner is built around that question. A marketplace usually isn't.
Programs evaluating clinical placement services can apply a short, practical checklist:
- Is vetting clinician-led? Someone with clinical judgment should be assessing fit, not just checking a box.
- Is the site approved separately from the preceptor? If only the individual is vetted, half the risk is unmanaged.
- Is there license-integrity screening with real disqualification? A standard with no teeth isn't a standard.
- Is verification ongoing, or one-time? Re-verification is what catches mid-rotation change.
- Is documentation a byproduct, or a scramble? If the records only get assembled before an audit, the process isn't built for accreditation.
A placement service that operates as an open listing tends to fail this checklist by design: it connects and steps back, leaving fit and proof to the program. That gap is exactly what NPHub's model is built to close, which is why it tends to read less like a vendor relationship and more like an extension of a program's own clinical infrastructure. The same standard applies whether the rotation is an NP preceptorship in family practice or a placement that overlaps with how other healthcare disciplines train, because the underlying discipline of confirming fit and documenting it doesn't change by specialty.
This is also the lens programs can use to weigh their own situation honestly. A nurse practitioner (NP) program with deep local relationships may need a partner only for hard specialties or thin geographies. A distance program may need structured capacity across the board. Either way, the evaluation is the same: not how fast a name appears, but how defensible the placement is once it does.
If your program is evaluating clinical placement support and wants a partner whose vetting actually verifies fit and stands up to accreditation review, talk with the NPHub university team. Book a call with our university partnerships team to map this to your cohort size, specialty mix, and graduation timeline.
Frequently asked questions
What makes clinical sites so hard to secure for NP students?
It's hard to secure because demand has outgrown the supply of clinicians willing to precept, and most placement efforts optimize for speed instead of fit. The same nurse practitioner preceptors get approached by multiple programs each term, and the thinnest pools, like psychiatric mental health, women's health, and rural areas, are exactly where a loose match is hardest to repair. The result is a process that feels harder every cohort, even when a program has reasonable access to clinical sites.
Does a preceptor matching service guarantee school approval?
No. A preceptor matching service can connect a student to a preceptor, but the introduction alone does not guarantee the placement will clear school approval. Approval depends on whether the preceptor's credentials, scope, and clinical site actually meet the program's requirements, which is a verification step many open-listing services leave to the program and student. A service that vets fit and approves the site upfront reduces the risk of a rejected rotation; one that simply makes introductions does not.
Why does strict vetting speed placement up rather than slow it down?
Strict vetting speeds placement up over time because it prevents the rework that rushed placements create. A match confirmed for scope, specialty, site, and documentation on the first attempt doesn't come back as a rejected rotation or a mid-rotation collapse that has to be solved again under deadline. Programs that skip vetting feel faster at booking and slower across the term, because they keep redoing placements that didn't hold.
What documentation do NP programs need for CCNE or ACEN?
NP programs need four things reviewers consistently ask for: preceptor qualification records (license, board certification, clinical experience), evidence that clinical sites were formally approved rather than just used, current signed affiliation agreements matched to active rotations, and proof of ongoing oversight across the full rotation. A single missing record is a clerical issue; a pattern of gaps across cohorts is what surfaces as a finding. The most defensible programs generate this documentation as placements happen rather than assembling it before a site visit.
Should NP students find their own preceptors?
Most programs that rely on student self-placement see uneven results. The model shifts the sourcing burden to the people with the least leverage, time, and visibility into compliance requirements, and it widens the gap between students with strong professional networks and those without. It also tends to produce inconsistent records that resurface during accreditation review. A dedicated, vetted placement function produces more equitable outcomes and more defensible documentation.
What's the difference between a placement marketplace and a placement partner?
A placement marketplace connects an available preceptor to a student and steps back, leaving fit, site approval, and documentation to the program. A placement partner treats those as its own responsibility: vetting clinical fit, approving the site separately from the preceptor, screening credentials, and maintaining the records a program can defend later. The simplest test is whether the service can prove a placement was sound, not just that it was made.
Find a preceptor who cares with NPHub
Book a rotation.webp)


.webp)

%20(3)%20(2).svg)