.png)



.webp)
TL;DR
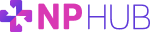
- Manual clinical placement is not free, its cost is just hidden. Because no one invoices a program for placement work, the expense disappears into faculty hours, delayed tuition cycles, accreditation remediation, turnover, and student out-of-pocket spend, where it never gets counted.
- The work is real labor absorbed into the wrong roles. Sourcing, follow-up, and paperwork get distributed across faculty and coordinators who were hired to teach and advise, so the true cost shows up as displacement: the high-value teaching and program work that did not happen.
- Delays carry a direct financial price. A slipped rotation pushes back graduation, tuition cycles, and licensure, and when programs run out of capacity, students often pay third-party agencies to secure a placement themselves.
- A structured process converts hidden labor into things a program can plan around. It replaces ad-hoc effort with capacity, speed, compliance, and reliability, building a repeatable system that compounds across cohorts instead of resetting to zero every term.
- Strict, clinician-led vetting is what removes the cost at the source. NPHub's process, clinician-led oversight, a structured NP-to-NP vetting interview, license integrity screening, separate clinical site approval, and 45-day re-verification close the gaps that create rework and faculty drain before they open.
Clinical placement rarely shows up as a line item in a program's budget. No one sends an invoice for the hours a faculty member spends emailing clinics, or for the weeks a cohort waits while a coordinator chases down one more preceptor. Because the bill never arrives in a recognizable form, manual clinical placement processes can feel essentially free. They are not. The cost is real, and it is being paid every term. It is simply distributed across places where no one is counting.
Those costs land in faculty hours redirected away from teaching, in graduations delayed when students cannot secure rotations on time, and in the accreditation exposure that builds quietly whenever documentation is assembled by hand. Manual processes do not remove the work of placement. They hide it inside roles that were never designed to absorb it, and the program pays for it later in burnout, delays, and remediation.
This blog post puts names and numbers to those hidden costs, what manual placement actually consumes, where the financial pressure shows up, and what a structured process replaces it with.
If your program is weighing the true cost of how clinical placement gets done today, the NPHub university team works with NP programs on exactly that question. Get in touch with our university team to talk it through.
What are the hidden costs of manual clinical placement processes?
The hidden costs of manual clinical placement are the resources a program spends on work that never produces an invoice. They show up as faculty and coordinator time, delayed tuition cycles, accreditation remediation, faculty turnover, and student out-of-pocket spending on third-party agencies. Because none of these appear as a placement line item, they are easy to miss and hard to manage.
Manual processes do not eliminate this work. They scatter it across people and budgets that were never set up to absorb it, which makes the true cost difficult to identify, harder to budget for, and nearly impossible to weigh in everyday decision making.
The hidden costs of manual clinical placement processes fall into five categories:
- Faculty and coordinator time: Hours spent on outreach, follow-up, and paperwork are valuable resources pulled away from teaching, curriculum, and student support.
- Delayed tuition cycles: When nursing students cannot secure rotations on time, graduations slip, and the tuition tied to on-time completion slips with them.
- Accreditation remediation: Records assembled by hand tend to be uneven, and that administrative burden comes due during CCNE or ACEN review.
- Faculty turnover: Sourcing work piled onto educators feeds burnout, and replacing experienced faculty carries a cost of its own.
- Student out-of-pocket spend: When a program runs out of capacity, students fill the gap themselves, often paying thousands per semester to secure a placement.
Some of these costs land on the institution, some on faculty, and some on students and their families. The missed opportunities, cohorts not grown, and faculty research not done rarely get counted at all. The sections below put numbers to each one.
Why do manual clinical placement processes cost more than they appear to?
Manual clinical placement processes cost more than they appear to because the work is real labor that has been absorbed into existing roles rather than budgeted as its own function. Nothing about a manual process is actually free. The hours are simply paid for by faculty, coordinators, and administrators out of time that was meant for teaching and student support, so the cost never appears where anyone would think to look for it.
This is the quiet mechanism behind hidden costs: the expense does not disappear; it relocates. When a school has no dedicated home for sourcing, the administrative tasks of placement, outreach to providers, follow-up, credential checks, and paperwork get distributed across people who were hired to teach, advise, and run clinical operations. Each task looks small in isolation. In aggregate, they pull meaningful capacity away from the work those roles exist to do, and they quietly shape day-to-day decision making about what gets attention and what gets dropped.
Three aspects of this cost make it easy to underestimate:
- It is unbudgeted: Because no one is invoiced for placement labor, it never competes for resources the way a line item would. It stays invisible until something breaks.
- It is fragmented: The work is split across many people in small increments, so no single person sees the full total, and the program never adds it up.
- It is measured in displacement, not spend: The real cost is the teaching, mentorship, and program development that did not happen because the time went to sourcing instead.
That displacement is the most expensive part, and the hardest to see. A faculty member chasing preceptors is not just spending an hour on outreach. They are losing an hour of the focus and clinical knowledge their training was built for, and the program loses the higher-value work that hour would have produced. The same hours that should support curriculum and mentorship are instead spent leading a manual search and completing forms, the kind of valuable resources a program cannot afford to spend twice.
Manual processes do not lower the cost of placement. They convert it into something a budget cannot capture, which is the key reason it keeps growing without anyone deciding to let it. A program that relies on this model is not saving money. It is paying in a currency it never tracks.
The administrative burden: How much time do faculty and coordinators spend on manual preceptor sourcing?
Manual preceptor sourcing consumes far more faculty and coordinator time than most programs account for, because it runs continuously beneath everything else they do. Every term, faculty and coordinators spend hours on outreach, follow-up, and credential checks, time pulled directly away from teaching, curriculum design, and student support, the work for which their training was actually built.
The volume is real. At the University of Southern California, the clinical placement team was setting 3 AM alarms to make coordination calls while carrying full teaching loads. That is not a story about one understaffed team. It is what manual sourcing looks like when the work has no dedicated home and falls to the people closest to it.
A few things make this time so costly:
- It displaces high-value work: Hours spent on administrative tasks are hours not spent on instruction, mentorship, or program development, the things faculty knowledge and credentials exist to deliver.
- It fragments focus: Sourcing rarely arrives as a scheduled block. It interrupts, which makes the surrounding teaching and advising work less effective too.
- It burns a resource that does not refill easily: Experienced faculty and coordinators are valuable resources, and their attention is finite. Spent on outreach, it is gone.
The deeper cost shows up in retention. The 2026 NSI National Health Care Retention Report puts the average cost of losing a single bedside RN at $60,090. Faculty are not immune to the same pressure, and the parallel is the point: when skilled people are worn down by work outside their core role, some leave, and replacing them is expensive. Every preceptor relationship a departing faculty member built tends to leave with them, so the program absorbs the cost twice, once to replace the person, and again to rebuild the sourcing capacity that walked out the door.
Protecting faculty and coordinator time is not a soft benefit. It is one of the clearest ways a program protects both its budget and the colleagues it depends on.
How do clinical placement delays turn into financial costs?
Clinical placement delays turn into financial costs the moment a rotation slips. A delayed rotation delays graduation, and a delayed graduation pushes back the tuition cycle, the licensure timeline, and the point at which a new nurse practitioner can start earning. When a program runs out of capacity entirely, students often absorb the cost themselves, paying several thousand dollars per semester to third-party agencies to secure a placement.
The numbers are not abstract. Students searching independently are routinely asked to pay $4,000 to $5,000 for a single semester placement covering roughly 250 hours of required, unpaid clinical training. That expense lands on people who are usually mid-career, balancing full-time work and families, and are least able to absorb a surprise bill on top of tuition.
The cost compounds in directions programs do not always trace:
- Delayed earnings: Every postponed term is a term the student is not yet working at an NP salary, a real loss for them and their family.
- Extended expenses: Tuition, living costs, and loan interest keep accruing while the clock runs, and the program's on-time completion metrics slip with each delay.
- Equity gaps: When access depends on the ability to pay, success starts tracking with bank balances rather than effort, which works against the diversity the profession is trying to build.
- Missed opportunities: Cohorts a program could have grown, and employers waiting on graduates it could have prepared, never materialize when placement is the bottleneck.
There is a reputational cost layered on top. Students talk, to peers, to prospective applicants, and to the employers who eventually hire them. A program known for placement instability has a harder time recruiting the next cohort and a harder time protecting the partnerships it depends on. The financial damage of manual placement does not stay contained to one delayed student. It moves outward into enrollment, reputation, and the program's standing for years.
What does a structured clinical placement process replace those costs with?
A structured clinical placement process replaces unpredictable, hidden labor with four things a program can actually plan around: capacity, speed, compliance, and reliability. While ad-hoc sourcing yields different results each term, depending on who handled it, a structured process applies the same standards every time. The work stops being a scramble and becomes a repeatable system.
The difference lies between effort and infrastructure. Effort resets to zero each term. A system compounds, building on the relationships, records, and processes already in place.
Here is what a structured process converts the hidden costs into:
- Capacity instead of scarcity: A continuous pipeline of vetted preceptors grows over time rather than restarting with each cohort, which steadily increases the number of students a program can place.
- Speed instead of delay: When preceptors are already sourced and verified, matching a student is a step in a process, not a months-long search, and rotations start closer to on time.
- Compliance instead of exposure: Documentation is captured as the work happens, so records are audit-ready by default rather than reconstructed under pressure.
- Reliability instead of volatility: Relationships that are actively maintained produce repeat preceptors, which support stability term over term.
None of this requires replacing a program's judgment over its own clinical curriculum. A structured process simply gives that judgment a dependable foundation to work from. The key shift is treating placement as integration into a program's operations, supported by clear systems and the right technology, rather than as a recurring problem the program has to resolve from scratch each time. Once that shift happens, the hidden costs stop accumulating, because the work that generated them is finally being done on purpose, by a function built for it.
How NPHub's vetting process removes the hidden cost of manual placement
NPHub removes the hidden cost of manual placement by treating vetting as the core of a structured process rather than a final checkbox. Most of the rework, rejected placements, and faculty drain in manual sourcing trace back to weak or inconsistent vetting. When every preceptor and site is evaluated to the same standard up front, the gaps that create downstream cost mostly close before they open.
The vetting itself is clinician-led, not administrative. It is built on five components:
- Clinician-led oversight: Every preceptor is sourced and vetted by an internal team of five board-certified nurse practitioners. Because the people making the call have practiced in similar settings, they can judge whether a preceptor's scope, patient population, and qualifications actually fit a given rotation, a clinical judgment, not a credential check.
- Structured NP-to-NP vetting interview: Each prospective preceptor completes a focused 20-minute conversation with a board-certified NP that confirms practice location, scope, specialty alignment, and the patient population a student will see, whether that is primary care, mental health, women's health, or another setting.
- Credential and license integrity screening: Active licensure, board certification, and professional background are verified directly, with zero-tolerance disqualification for any disciplinary action or restriction. This protects students, programs, and the patients involved.
- Clinical site approval: The site is vetted separately from the individual preceptor, confirming that the practice, clinic, or health system can administratively support a placement and complete the documentation a program requires.
- 45-day re-verification: Active preceptors and sites are re-checked every 45 days, because practice settings, schedules, and patient populations change. Continuous monitoring catches those shifts before they become mid-rotation problems.
Together, these components do for a program what manual sourcing cannot: they apply a single, consistent standard across every provider, site, and cohort. That consistency is what programs and universities can rely on, and it is what turns placement from a recurring cost into dependable infrastructure. It also extends across the range of settings NP students train in, from independent practices to hospitals and larger health systems, and the organizations and communities they serve.
If your program is weighing the true cost of how placement gets done today, the NPHub university team works with NP programs to map a structured approach to their cohort size, specialty mix, and graduation timeline. Get in touch with our university team to start that conversation.
Frequently asked questions
What is the true cost of manual clinical placement for an NP program?
The true cost of manual clinical placement is mostly hidden, paid in faculty and coordinator hours, delayed tuition cycles, accreditation remediation, faculty turnover, and student out-of-pocket spending rather than in a single invoice. Because the work is absorbed into existing roles instead of budgeted, programs rarely see the full total. The clearest way to measure it is to add up the time skilled staff spend on sourcing and the high-value teaching and program work that time displaces.
Why is manual clinical placement so time-consuming for faculty and staff?
Manual placement is time-consuming because sourcing, follow-up, and documentation are repeated by hand every term, with no system carrying the work forward. Much of that time goes to redundant data entry, the same preceptor and site details re-keyed across forms and platforms, which wastes hours that healthcare and academic teams could spend elsewhere. A structured process captures information once and reuses it, which is where most of the time savings come from.
What documentation do NP programs need for each clinical placement?
Each clinical placement typically requires a signed affiliation agreement between the academic institution and the clinical site, verified preceptor credentials, and student compliance records. On the student side, that usually includes passing a background check and providing immunization records, and in many cases a current Basic Life Support (BLS) or Advanced Cardiovascular Life Support (ACLS) certification. When these records are assembled manually, gaps and version-control errors are common, which is what creates accreditation exposure later.
How does manual data handling create compliance risk?
Manual data handling creates compliance risk because sensitive student and preceptor information moves through email, spreadsheets, and paper forms that were never built to protect it. Every manual transfer of licensure details, immunization records, or background checks increases the chance of a gap, an error, or a data breach. A structured process reduces that exposure by keeping records in one consistent, audit-ready system rather than scattered across inboxes.
What is a clinical placement, and what do students actually do during one?
A clinical placement is a supervised learning experience in which a healthcare student completes required hours at an approved clinical site under a qualified preceptor. During a placement, NP students perform direct patient care tasks, history-taking, assessment, diagnosis, and management, under close supervision, building the competencies their program and licensure require. The placement is where classroom learning becomes applied clinical practice.
How do programs make sure placements match their educational goals?
Programs align placements with educational goals through competency-based education, which maps each rotation to the specific core competencies a student must demonstrate. A placement is not just any available site; it is one whose scope, patient population, and supervision support the competencies the program is accountable for. Vetting the site and preceptor against those goals up front is what prevents a rotation from being rejected or judged inadequate later.
Is a structured placement process worth it for a smaller NP program?
Yes, and smaller programs often feel the strain of manual placement most acutely because they have fewer faculty relationships to draw on. When a single coordinator or a few faculty members handle all sourcing, every hour lost to it represents a larger share of the program's total capacity. A structured process protects that limited capacity, which is frequently more valuable to a small program than to a large one.
Does moving away from manual sourcing reduce faculty workload?
Yes. Moving sourcing, vetting, and documentation to a dedicated structured function returns faculty time to teaching, mentorship, and curriculum, the work their training was actually designed for. It also reduces the burnout and turnover risk that builds when educators absorb administrative work outside their role, which protects both the faculty and the preceptor relationships they would otherwise take with them if they left.
Find a preceptor who cares with NPHub
Book a rotation.webp)

.webp)


%20(3)%20(2).svg)