.png)



.webp)
TL;DR
- Clinical placement complexity compounds; it does not scale linearly. A program that doubles enrollment multiplies its placement workload across more specialties, more states, more affiliation agreements, and more documentation surface area, not just more rotations.
- Faculty burnout and accreditation exposure are the same problem. When sourcing has no dedicated home, faculty absorb the work, documentation thins, and CCNE or ACEN reviewers eventually identify gaps that were invisible at a smaller scale.
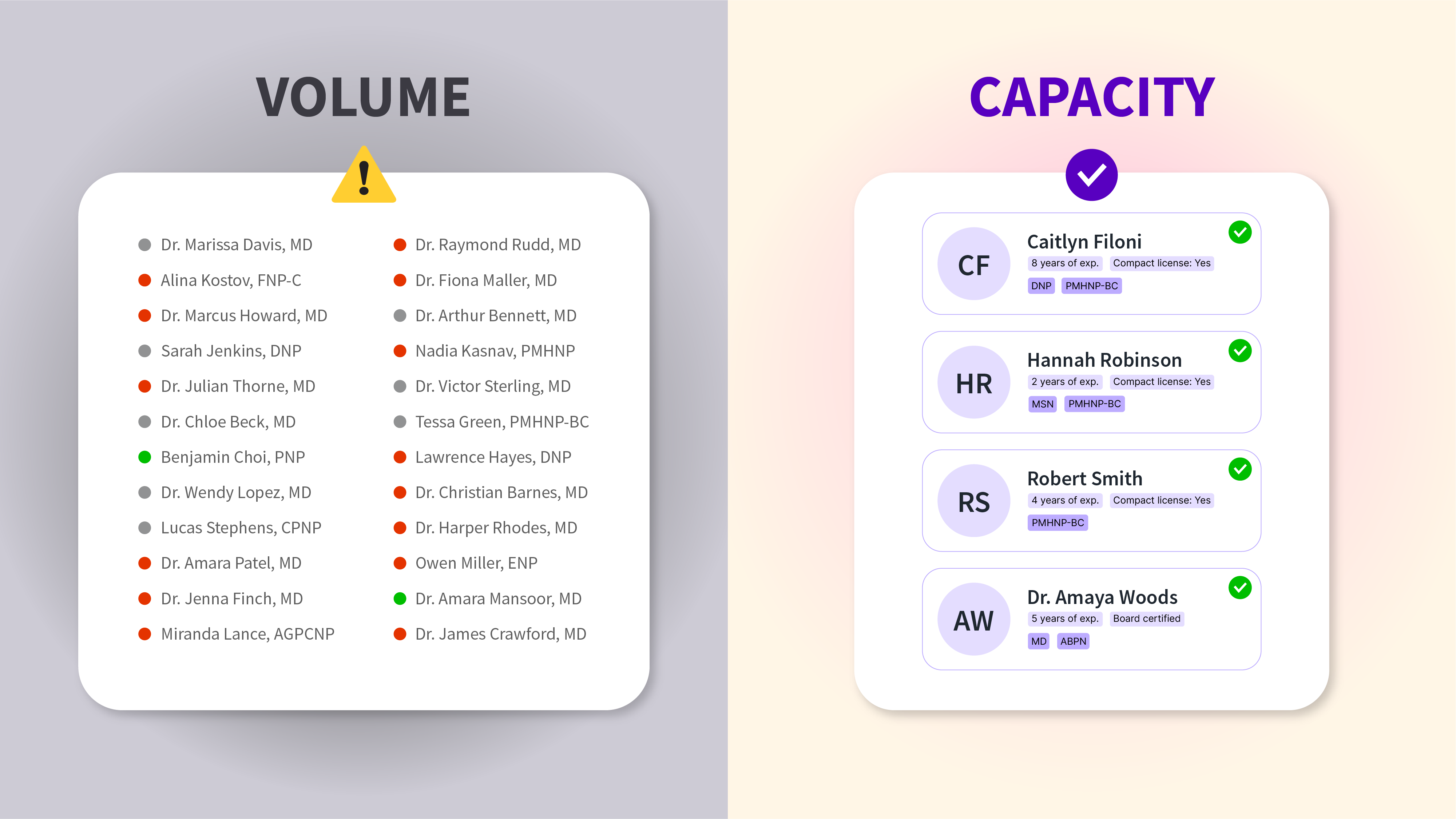
- Preceptor recruiting is a discipline, not a task. Recruiters operate upstream at the supply layer, sourcing and vetting at scale. Coordinators operate downstream, managing logistics once preceptors are secured. Most programs are short-staffed on the recruiting side because the work gets absorbed into coordination by default.
- The programs that scale cleanly treat placement as infrastructure. Continuous sourcing, clinician-led vetting, separate clinical site approval, audit-ready documentation, and ongoing re-verification, these are the operating characteristics that hold up as complexity compounds. NPHub's preceptor recruiting function is built around exactly these principles, with five operational pillars designed for the failure modes scaling produces.
- Mapping growth over the next three to five years? The conversation about clinical capacity benefits from happening early. Get in touch with the NPHub university partnerships team to discuss what scaling responsibly looks like across your cohort size, specialty mix, and geographic footprint.
Growth is the strategic priority across nurse practitioner education. The executive ambition is well-defined:
- Larger cohorts and expanded enrollment
- Distance learning and online program expansion
- New advanced practice specialty tracks
- Broader geographic reach into other states
The demand from working nurses pursuing graduate nursing careers continues to climb. The question here is whether the operating model underneath that growth was built to support it.
Most NP programs are still managing clinical placement using a model designed for a smaller, more local, more predictable era. It assumes faculty can absorb sourcing work between teaching obligations. It assumes clinical partners are within driving distance. It assumes documentation can be assembled when the accreditation review approaches. None of those assumptions holds as a program scales.
Here is the part that most NP programs underestimate when discussing scaling: clinical placement complexity does not scale linearly with enrollment. It compounds. A program that doubles its cohort size does not double its placement workload, it multiplies it across more specialties, more clinical sites, more states with their own approval process and compliance requirements, more affiliation agreements to maintain, and more documentation to defend under accreditation standards. Linear effort against compounding complexity is exactly how faculty burn out, and exactly how accreditation findings appear.
This article is an executive-level look at why scaling an NP program forces a rethink of clinical placement as infrastructure rather than logistics and why the underestimated discipline of preceptor recruiting is what separates programs that scale cleanly from programs that scale into crisis. The cost of getting it wrong shows up in delayed graduations, faculty turnover, and weakened program reputation. The cost of getting it right is the capacity to grow responsibly without compromising the quality of nursing education that the institution was built to deliver.
For NP programs already mapping the next three to five years of growth, the conversation about clinical capacity is one that benefits from happening early. The NPHub university team works directly with programs at exactly that stage.
Why Does Clinical Placement Management Complexity Grow Faster Than Enrollment?
Clinical placement complexity grows non-linearly because each additional student introduces compounding variables rather than additive ones. Specialty mix, geographic spread, preceptor availability, site approval cycles, and documentation depth all multiply against each other rather than stack. Doubling enrollment can triple or quadruple the operational load on a clinical placement team, especially when scaling nurse practitioner programs also involves expanding into distance learning or adding new advanced practice specialty tracks.
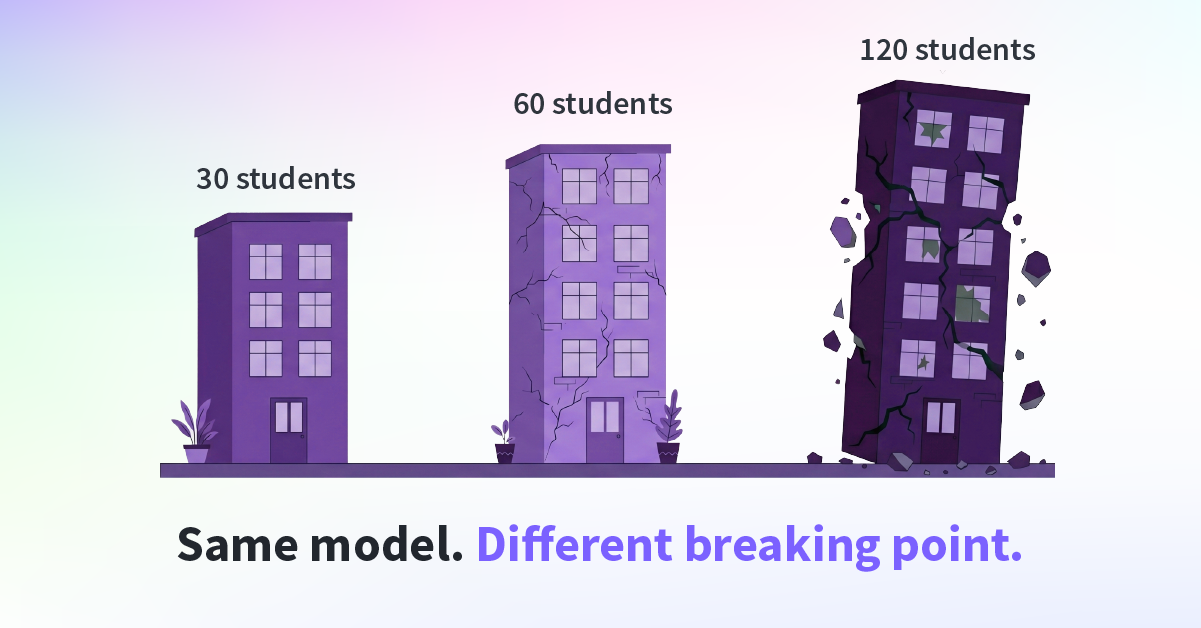
The math is worth slowing down on. Most leadership conversations about enrollment growth treat placement workload as roughly linear: more students means proportionally more rotations to coordinate. The lived experience inside a clinical placement office tells a different story. The capacity worked at 30 students breaks at 60, and breaks worse at 120.
Six variables compound against each other:
- Cohort size: More students means more concurrent rotations, more parallel preceptor relationships, and more potential failure points per term.
- Specialty mix: A program offering FNP, AGNP, PMHNP, and women's health is recruiting across multiple clinical communities with different scopes, settings, and acuity profiles.
- Geographic spread: Online and distance learning models distribute students across regions, each with its own healthcare landscape and provider availability.
- Site approval cycles: Every new clinical site requires its own administrative approval, affiliation agreement, and onboarding documentation.
- Documentation depth: More placements mean more records to maintain, refresh, and produce on demand under accreditation review.
- Relationship maintenance: Preceptors are not one-time contacts; sustaining the network across cohorts requires ongoing engagement that grows with every new clinical partner added.
Any one of these is manageable in isolation. The compounding effect is what produces the operational strain administrators describe.
The national data backs this up. The American Association of Colleges of Nursing reported that in 2024, a total of 80,162 qualified applications were not accepted at schools of nursing nationwide, and named insufficient clinical placement sites, faculty, preceptors, and classroom space as the primary barriers to accommodating qualified applicants. Workforce demand is climbing. The infrastructure underneath nursing education has not kept pace.
Cisive's 2026 Clinical Placement Benchmark Report found that 30% of administrators identify clinical placements as the least efficient part of their program, more than any other area, even when academic components are running smoothly. More telling for executive readers: more than 90% of programs report that challenges in securing enough clinical placements have at least some impact on their operations.
Programs cannot solve a problem of compounding complexity with linear effort. Adding one more coordinator, asking faculty to absorb additional outreach, or expecting students to self-source at greater volume does not address the underlying mechanics. It pushes the breaking point out by one or two cohorts.
What Changes When an NP Program Scales?
When NP programs scale, four operational realities shift at the same time: cohort size, specialty diversification, geographic distribution, and compliance surface area. Each shift independently increases placement complexity. Together, they break the assumptions on which the original placement model was built, and they rarely break in isolation because growth in one dimension typically triggers growth in the others.
Cohort Size Growth
Larger cohorts do not just produce more placements per term. They produce more concurrent rotations running in parallel, more preceptor relationships to manage at the same time, more documentation cycles overlapping, and more failure points per term. A clinical placement office that comfortably handled 20 students per cycle is not 3x as strained at 60 students, it is functionally a different operation, with different tools, staffing, and process requirements.
The compounding piece often goes unnoticed in planning conversations. Every additional student increases the probability that at least one rotation will encounter a disruption, a preceptor schedule change, a site capacity shift, or a documentation gap. At a small scale, those events are exceptions handled individually. On a larger scale, they become a continuous baseline of incidents that the placement team is always managing.
Specialty Diversification
Most growing NP programs do not just enroll more students. They expand the specialty tracks they offer. Adding FNP, PMHNP, AGNP, women's health, pediatrics, or acute care means recruiting across multiple clinical communities, each with different scopes of practice, patient populations, acuity profiles, and unique requirements for what counts as an appropriate clinical setting.
The sourcing differs track by track. A family nurse practitioner pathway can often find preceptors in community primary care practices, federally qualified health centers, and rural clinics. A psychiatric mental health NP track is recruiting from a much smaller pool of providers, often concentrated in specific settings, and frequently in higher demand from competing programs. Pediatric tracks face similar supply constraints. Recent research on NP preceptor motivators reinforces this: significant differences exist in what motivates FNP, PMHNP, and PNP preceptors to participate, suggesting that recruiting strategies cannot be applied uniformly across specialties.
Treating all specialty tracks as a single sourcing problem is how programs end up with capacity gaps that recur every term. They are not the same problem.
Geographic Distribution
Online and distance learning expansion is the change that breaks local-network sourcing most decisively. When students live across multiple states, every placement becomes a multi-jurisdictional operation. Each state has its own approval process, its own board of nursing regulations, and its own compliance requirements for out-of-state programs placing students within its borders.
Many institutions already maintain detailed state-by-state authorization charts because the regulatory landscape varies significantly: some states require additional approvals, some restrict enrollment outright, and some require specific reciprocity arrangements, such as NC-SARA membership. The administrative work of confirming a placement is compliant in a given state is substantial. The administrative work of doing it across thirty states simultaneously is a different category of operation.
Faculty networks and alumni connections, the relational infrastructure most programs built their placement model around, were never designed to span this much geographic distribution. The model assumes proximity. Distance learning eliminates that assumption.
Compliance Surface Area
The fourth shift is the one that most directly drives accreditation exposure. More placements multiplied by more states multiplied by more clinical sites multiplied by more preceptors equals exponentially more documentation to maintain. Affiliation agreements compound. Credentialing cycles overlap. Background checks and immunization records multiply. Every additional placement is another set of records that must be current, retrievable, and defensible under review.
This is the mechanic that turns a manageable accreditation posture into a fragile one. Documentation gaps that were invisible at a small scale become statistically inevitable at a larger scale unless the underlying process is rebuilt to handle the volume. CCNE and ACEN reviewers do not need every record to be perfect. They need the process to be repeatable, and demonstrating repeatability becomes harder as the compliance surface area expands.
These four elements rarely arrive one at a time. A program adding distance learning is usually also adding cohort size, often introducing new specialty tracks, and almost always increasing the compliance surface area in the process. Growth strategies treat them as separate initiatives. Operations experiences them as one compounding problem.
For NP programs already mapping how multiple shifts will land at once over the next several cohorts, the NPHub university team regularly works through these tradeoffs with deans and program directors, what is already straining, what is holding up, and where dedicated recruiting infrastructure would change both. It tends to be a useful conversation to have before the next admissions cycle locks in the next layer of growth.
Why Does Faculty Burnout Accelerate as NP Programs Scale?
Faculty burnout accelerates during scaling because sourcing work that was absorbable at small cohort sizes becomes unsustainable as complexity compounds. When clinical placement sourcing has no dedicated home, faculty absorb the workload on top of teaching, mentorship, research, and curriculum design, and the work that suffers first is the work the institution hired them to do.
- Lost teaching time that erodes the quality of nursing education in ways that compound across cohorts.
- Reduced research output, which weakens the program's reputation and standing within collegiate nursing education.
- Faculty turnover, which exports preceptor relationships out the door with every departure.
The turnover piece carries the most institutional risk. The 2026 NSI National Health Care Retention Report found that the cost of losing a single bedside RN reached an average of $60,090. Nursing programs are not insulated from the same dynamics inside their own faculty ranks.
USC's experience is the perfect example. Before bringing in outside support, USC's small clinical team was setting 3 AM alarms to coordinate placement calls across time zones, including a student in Guam, while maintaining full teaching loads. Dr. Cynthia Sanchez, USC's Clinical Placement Coordinator, put it directly:
"Finding placements isn't a normal faculty job. And also, finding that time again to call places that are all over the country. We even had a student who was in Guam."
That is the structural insight executive leaders eventually arrive at. Faculty burnout during scaling is the predictable outcome of asking faculty to do work that is not part of their role, was not part of their training, and does not fit within the time available for their actual responsibilities. Programs that recognize this early protect their faculty's capacity to do the work they were hired to do.
What Does a High-Performing Preceptor Recruiting Function Look Like at Scale?
A high-performing preceptor recruiting function operates continuously rather than seasonally, applies clinician-led judgment to fit and teaching readiness, separates clinical site approval from individual preceptor verification, and maintains audit-ready documentation by default. The orientation is pipeline-driven, not deadline-driven which is exactly the orientation that compounding complexity requires.
The operating characteristics are recognizable across the programs doing this well:
- Continuous outreach, not seasonal scrambling.
- Clinician-led vetting, applying clinical judgment rather than credential checking.
- Site approval treated as distinct from preceptor approval.
- Documentation generated as a byproduct of process, not assembled retroactively.
- Relationships maintained across cohorts, not rebuilt each term.
- Specialty depth across the rotations programs actually need, primary care, family practice, women's health, psychiatric mental health, pediatrics, and acute care.
NPHub's recruiting function is built around five operational pillars that map directly to the failure modes scaling produces. Each pillar exists because a specific question keeps surfacing in conversations with NP programs hitting the limits of their existing model.
- Clinician-led oversight: Board-certified NPs source and vet every preceptor, because evaluating fit across specialties is a clinical judgment, not an administrative one.
- Structured NP-to-NP vetting interview: A 20-minute peer-level conversation evaluates scope, specialty alignment, patient population, and readiness to teach, because licensure alone does not determine whether a preceptor can deliver a meaningful clinical experience.
- Credential and license integrity screening: Active licensure, board certification, and disciplinary history are reviewed for every advanced practice clinician, with zero-tolerance disqualification for license issues. Background checks and ongoing credential verification hold up across hundreds of concurrent placements.
- Clinical site approval: Sites are approved separately from individual preceptors, because a qualified clinician at an unviable site still produces a failed rotation.
- 45-day re-verification: Active preceptors and sites are re-checked every 45 days, because clinical environments shift mid-rotation and careful oversight cannot stop at onboarding.
This is the difference between a placement vendor and clinical capacity infrastructure. Programs ready to evaluate what that distinction would mean operationally can get in touch with the NPHub university partnerships team to discuss what scaling responsibly looks like across their cohort size, specialty mix, and geographic footprint.
What Does This Look Like in Practice? Two Programs that Rebuilt Their Placement Model for Scale
Both started with small clinical placement teams trying to manage growing complexity. Both arrived at the same structural conclusion: capacity has to be built around the program, not absorbed inside it.
Graceland University: From a 2-Person Team to a 51-Person Extension
Graceland offers a full slate of online NP programs across Adult & Gerontology Acute Care, Family NP, and Psychiatric Mental Health tracks. With a small two-person clinical placement team limited to home-state sourcing, frustrated students were skipping a semester or two waiting for placements to materialize.
Partnering with NPHub gave Graceland access to a vetted network of 2,000+ active preceptors across 45 states, plus a dedicated preceptor-recruiting team that sources exclusively for Graceland students. The result: a 100% reduction in NP student stop-outs due to placement, down from 10 students per semester to 0.
"Having NPHub actually go out there and essentially take my 2-man team and make it a 51-man team is HUGE." — Lisa Winch, Graduate Practicum Coordinator
University of Southern California: Eliminating 3 AM Coordination Calls
USC supports NP students nationwide and internationally. The placement footprint was the problem, faculty were setting 3 AM alarms to coordinate calls across time zones while maintaining full teaching loads.
The partnership expanded USC's two-person clinical team into access to a 60+ preceptor-expert workforce. Faculty returned to teaching. Geographic locations that were previously impossible became reachable.
"Finding placements isn't a normal faculty job." — Dr. Cynthia Sanchez, Clinical Placement Coordinator
Both programs reached the same conclusion: faculty are educators, recruiting at scale is a different discipline, and separating the two protects student progress and program reputation.
What Should Executive Leaders Prioritize When Rethinking Placement for Scale?
Executive leaders should prioritize five strategic shifts: separating recruiting from coordination, building capacity ahead of enrollment, treating documentation as continuous, evaluating partners on clinical judgment, and measuring placement infrastructure on the same time horizon as faculty hiring and curriculum design. Each shift moves clinical placement out of the operational margin and into the strategic core where it belongs.
- Separate recruiting from coordination: These are different disciplines with different time horizons. Coordination is reactive and deadline-driven. Recruiting is proactive and pipeline-driven. When the same person owns both, recruiting consistently loses to the urgent, which is how capacity gaps quietly compound across cohorts.
- Build capacity ahead of enrollment: Admissions projections should be matched to pipeline depth, not the other way around. Programs that admit larger cohorts on the assumption that placement will catch up are essentially borrowing capacity from future cohorts. The interest comes due in delayed graduations and faculty burnout.
- Treat documentation as continuous: Audit-ready by default, not assembled before reviews. The compliance burden during scaling is not just a larger volume; it is the loss of margin for error. Continuous documentation is what makes repeatability defensible under CCNE and ACEN reviews and reduces the remediation work that would otherwise flow back to faculty.
- Evaluate partners on clinical judgment, not marketplace volume: Marketplaces fill slots. Recruiting partners evaluate fit. The distinction matters most at scale, because volume without judgment produces placements that satisfy the headcount but fail the educational mission. The right partner is staffed with clinicians who can assess scope, acuity, and teaching readiness, not just verify credentials.
- Measure on long horizons: Placement infrastructure is a multi-year investment, not a per-cohort line item. The programs that scale cleanly treat clinical capacity the same way they treat faculty hiring, curriculum design, and research investment, as durable infrastructure that compounds in value over time and has a significant impact on long-term program health.
These priorities are essential because they reframe what clinical placement actually is. It is the operational infrastructure that determines whether a program can deliver on the future it is recruiting students into.
For programs ready to map these priorities to their own cohort size, specialty mix, and geographic footprint, the NPHub university team regularly engages in this exact conversation with deans and program directors leading change within their institutions.
Frequently Asked Questions
1. How do NP programs scale clinical placement capacity without adding faculty?
Programs scale capacity without adding faculty by separating sourcing work from faculty responsibilities and assigning it to a dedicated recruiting function — internal or partnered. Faculty stay focused on teaching, mentorship, and curriculum, while a recruiting team builds a continuous pipeline of vetted preceptors. The result is more placements per cohort without expanding faculty headcount or eroding the academic mission.
2. What is the difference between a preceptor recruiter and a clinical coordinator?
A preceptor recruiter sources, vets, and onboards new preceptors at scale, operating upstream at the supply layer. A clinical coordinator manages the logistics of placements once preceptors are secured, scheduling, documentation, and student communication during active rotations. Both roles are necessary, and most programs are short-staffed on the recruiting side because the work gets absorbed into coordination by default.
3. How does program growth affect CCNE and ACEN accreditation exposure?
Growth increases accreditation exposure because ad-hoc sourcing produces inconsistent documentation, and inconsistencies that were invisible at a small scale become patterns at a larger scale. CCNE and ACEN reviewers examine repeatability across cohorts, not just outcomes, so documentation gaps multiply with cohort size and geographic spread. Programs scaling without rebuilding their documentation process for the new volume typically discover the exposure during the next review cycle.
4. What documentation do NP programs need to maintain across distance learning placements in multiple states?
Programs need to maintain preceptor qualification records (license, board certification, clinical experience), signed affiliation agreements with each clinical site, evidence of clinical site approval separate from individual preceptor approval, clinical clearance documentation including background checks and immunizations, and ongoing oversight records demonstrating information was refreshed during the rotation. Each state may also have its own approval process and compliance requirements that need to be documented. Records should be produced on demand for any cohort.
5. How long does it take to build a scalable preceptor pipeline?
Building a durable, scalable pipeline can take months of consistent outreach, depending on specialty mix, geographic concentration, and the existing preceptor base. Pipelines built reactively rarely become reliable because each placement cycle restarts from a near-zero state. Programs scaling cohort size should begin pipeline investment at least two cohorts ahead of the projected growth.
6. What should universities look for in a clinical placement partner when scaling?
Universities should seek clinician-led vetting, transparent screening of credentials and license integrity, separate approval of clinical sites and individual preceptors, ongoing re-verification rather than one-time onboarding, and audit-ready documentation generated as a byproduct of the process. The signal that distinguishes a partner from a vendor is whether their process is built to support program requirements and accreditation review, or simply to fill placement slots.
7. Can preceptor matching services support programs across multiple states and specialties?
Yes, when the service applies consistent vetting and documentation standards across every placement and operates with specialty depth, not just geographic breadth. Services that rely on open listings or basic credential checks typically struggle at scale, because volume without judgment produces placements that satisfy headcount but fail educational fit. The right partner maintains specialty-specific pipelines across primary care, family practice, women's health, psych mental health, pediatrics, and acute care.
8. How does ongoing preceptor re-verification protect program reputation during scaling?
Ongoing re-verification detects changes in a preceptor's license status, scope of practice, patient population, or clinical setting before they disrupt student rotations. A preceptor who was a strong fit at the start of the term may not be by week six as schedules shift and patient mix evolves. Continuous re-verification protects completed clinical hours, reduces last-minute placement scrambles, and produces the living audit trail that accreditation review and program reputation both depend on.
Find a preceptor who cares with NPHub
Book a rotation.webp)

.webp)


%20(3)%20(2).svg)